
An angry father's guide to vaccines
An angry father's guide to vaccines
Don't be like me, do your research first

Men of science have made abundant mistakes of every kind; their knowledge has improved only because of their gradual abandonment of ancient errors, poor approximations, and premature conclusions.
— George Sarton, founder, History of Science Society
(I’m not a doctor, this is my opinion.)
LAFAYETTE, California—The message that vaccines are safe and effective made perfect sense to my wife Lisa and me. Our beautiful boys would be fully vaccinated. I’d been vaccinated, and my wife had been vaccinated. It was the easiest decision two parents could make. You even get to kill two birds with one stone: protect your babies from infectious disease and contribute to herd immunity, and so protect others. What was the risk of something bad happening from a vaccine? The number thrown around—and still in wide use today—was “one in a million.”
Losing faith in my pediatrician and ultimately the entire medical establishment triggered a massive case of cognitive dissonance for me, as it does for so many parents who trusted their pediatricians with their children’s lives. Could my pediatrician be leading me astray? Could these vaccines really be harming my son? Are those crazy parents actually right? It’s an alienating, disturbing, troubling path that many autism parents must walk. In many cases the parents of children with autism were the most compliant when it came to mainstream medical care—our children typically received every vaccine and medical intervention recommended to us by our trusted doctors. We’re not “anti-vaxxers”; we’re mostly “ex-vaxxers,” the compliant parents who learned the hard way.
Few parents know how recent our high-volume vaccine program really is (I certainly didn’t), how different the US vaccine schedule is from many other first-world countries, how low US vaccination rates for children were as late as the 1980s (without any deadly epidemics), the wide range of side effects (“vaccine injury”) vaccines can create, the straightforward published science that shows vaccines are the culprit of an epidemic of autoimmune conditions (asthma, food allergies, etc.), or the fact that public health officials are well aware that clean water, sanitation, plumbing, and refrigeration had a much larger impact on infectious disease prevention than vaccines. There were so many things I didn’t know when I let my boys get all their vaccines; it’s hard to shake feelings of guilt for not doing my homework.
The 70s most vaccinated child? Me.
I grew up a "Military Brat" and always figured I must have been one of the most vaccinated kids of the 1970s. Born in May of 1969, I lived in Singapore (where I was born), Laos, Mexico, and Korea before I was ten and also traveled to Thailand, Malaysia, Hong Kong, Japan, and the Philippines during this same time period.
If you took a travel itinerary like that to your pediatrician today, he'd back up the vaccine truck and start pumping you and your child full of every vaccine he had in inventory and probably special order some unique ones, too.
I often heard my own son's pediatrician talk about "deadly foreign diseases" being "only a plane ride away" as he sought to allay our concerns over the volume of vaccines being given to our own kids.
I've never been able to find a vaccine schedule before 1983, but you'd sure think my own experience would be at the extreme upper end of vaccines given to a child. Not only did I live in multiple foreign countries, but I was also part of the tight military healthcare system where mandatory doctor visits are part of any overseas travel protocol. They could never miss me!
So, here's my schedule, my parents still had it.
To keep it simple, I am only listing my vaccines from birth to age 6 so I can compare it to today's schedule:
March 1970: Oral Polio
July 1970: Measles (Rubeola)
Sep. 1970: DPT
April 1974: Oral Polio
April 1974: Typhoid
That's it. I got 5 vaccines.
Today's kids get 36 in the same time period. And, these are typical American kids who may never leave this country. I had lived in or visited nine countries, a number of them third world!
Notable that my first vaccine was given when I was 10 months old. Once, I got 2 vaccines in the same visit. Otherwise, they were a minimum of 4 months apart, and in some cases YEARS apart.
What can we learn from one kid's vaccine schedule? The insane US vaccine schedule is something very, very new. (If a child of the 1970s can survive nine foreign countries with 5 vaccines, surely we can reduce the number of vaccines being given without putting our children and military at risk.)
Safe and effective, or profitable and who knows?
I’ve personally studied the US vaccination program for more than twenty years, looking for clues that might help me better understand what exactly happened to my son. After all, how can I help him get better if I don’t know what hurt him? Mind you, even saying that confuses some people; there’s just not a lot of awareness of the extreme and long-term side effects vaccines can cause in certain children. Much of what you hear in the mainstream media is actually public relations and spin expertly placed there by vaccine makers.
The “safe and effective” message repeated over and over again is a marketing message, but is not fully fact based. Consider the American Academy of Pediatrics (AAP), an organization typically quoted anytime a discussion of vaccines takes place. Is the AAP a benevolent, objective advocate for your baby? No, they are a trade union for pediatricians, and pediatricians generate the majority of their income from, you guessed it, vaccines. What about the nation’s keeper of the vaccine program, the CDC? Do they give parents objective information about the risks and benefits of vaccines? Or do they feel entitled to scare the heck out of the public to induce them to get vaccinated?
Most people have at least a little bit of cynicism when it comes to the pharmaceutical industry. Approval ratings for “Big Pharma” aren’t much higher than for members of Congress. A journal study published in 2013 titled, “Undue industry influences that distort healthcare research, strategy, expenditure and practice: a review” by University College London researchers looked carefully at how the pharmaceutical industry influences medical research, policy, and practice. What they found won’t surprise you too much:
To serve its interests, the industry masterfully influences evidence base production, evidence synthesis, understanding of harms issues, cost-effectiveness evaluations, clinical practice guidelines and healthcare professional education and also exerts direct influences on professional decisions and health consumers. . . . As a result of these interferences, the benefits of drugs and other products are often exaggerated and their potential harms are downplayed, and clinical guidelines, medical practice, and healthcare expenditure decisions are biased.
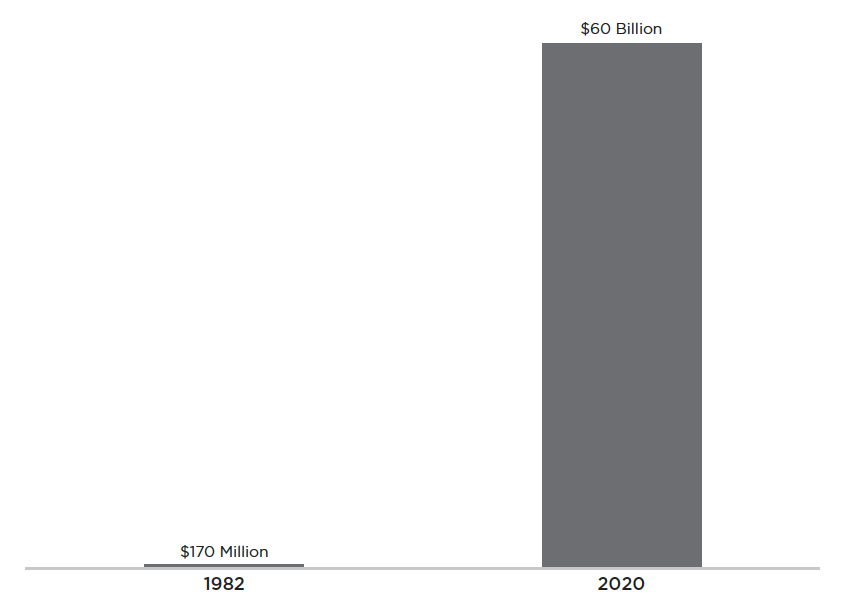
Some people mistakenly think vaccines don’t produce the same profit motivation as other products for pharmaceutical companies, but they do. What if I told you that the market for vaccines was worth $60 billion in 2020, up from $170 million in the early 1980s? That’s a 350-fold increase in revenues for vaccine makers in the last thirty years! And it’s not just vaccine makers who will manipulate the facts to serve their interests; they are joined by a federal agency that Robert F. Kennedy Jr. has described as a “captive agency” of the pharmaceutical industry, the CDC.
Inducing Fear, Anxiety, and Worry
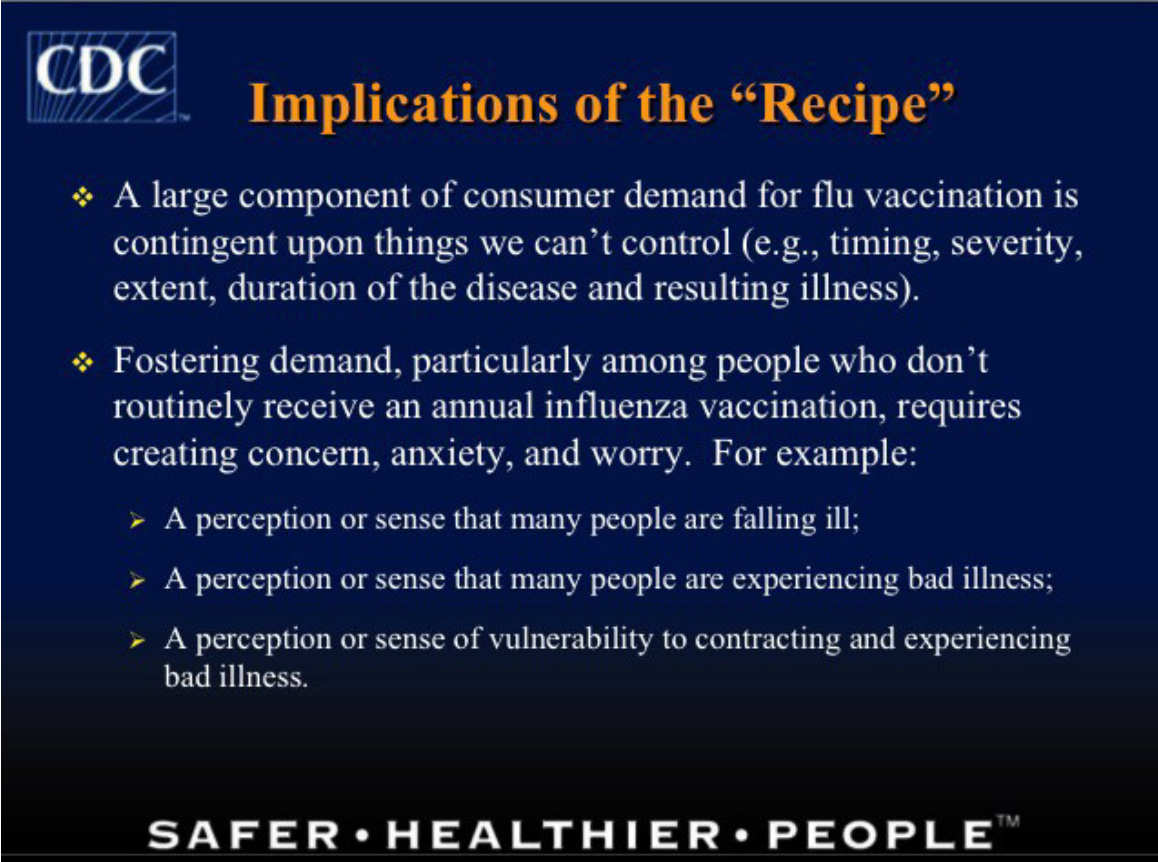
On April 14, 2004, Glen Nowak, an employee of the CDC, addressed his public health colleagues at the National Influenza Vaccine Summit in Atlanta, Georgia. The conference, cosponsored by the CDC and the American Medical Association, was filled to capacity in the Noble Ballroom of the tony Crowne Plaza Buckhead with public health officials, doctors, and representatives of the world’s largest vaccine makers.
Mr. Nowak’s presentation, entitled “Increasing Awareness and Uptake of Influenza Immunization,” provided insight into the mind-set of American public health officials.As the director of media relations for the CDC, Mr. Nowak told the crowd he considered his job to be to promote “concern, anxiety, and worry” amongst the general population, especially with people who “don’t routinely receive an annual influenza vaccination.” Want more people to get vaccinated? Demand will come from a “perception or sense of vulnerability to contracting or experiencing bad illness,” Mr. Nowak explained. During his speech Mr. Nowak made it clear that without provoking anxiety you won’t get the behavior you want:
The belief that you can inform and warn people, and get them to take appropriate actions or precautions with respect to a health threat or risk without actually making them anxious or concerned. This is not possible. . . . This is like breaking up with your boyfriend without hurting his feelings. It can’t be done.
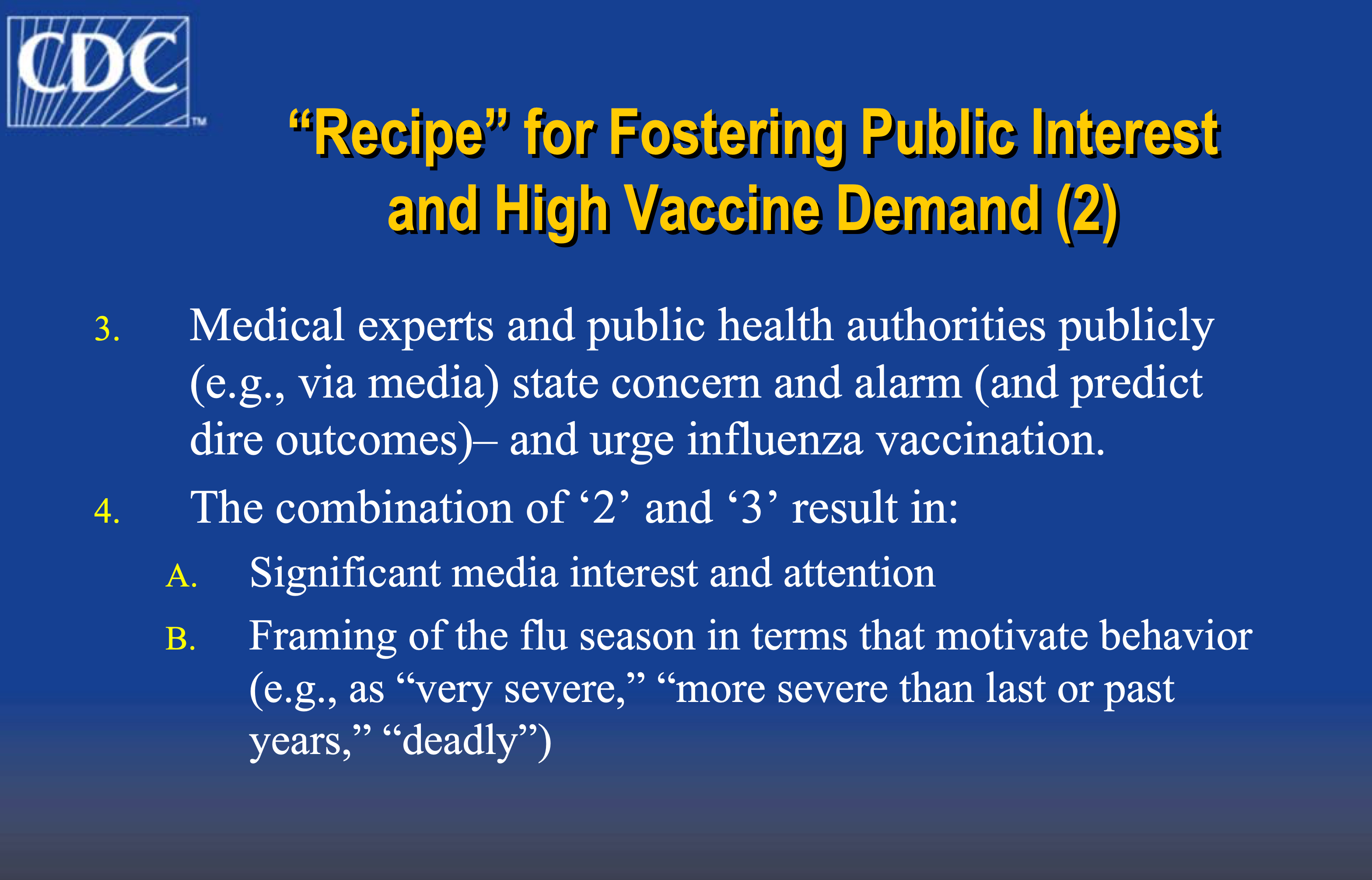
Mr. Nowak’s presentation included a “recipe” for creating high vaccine demand. Step #3 of Mr. Nowak’s seven-step recipe stressed the importance of medical experts and public health officials stating “concern and alarm” and predicting “dire outcomes” if people don’t get vaccinated. It’s critical spokespeople frame the flu season in ways that motivate behavior, Mr. Nowak explained, like “very severe” and “deadly.” References to “pandemic influenza” from the early 1900s might also help scare the populace into acting, he noted.
A few years later GlaxoSmithKline (GSK), a London-based vaccine maker, would brag to this same crowd that they had invested more than two billion dollars in flu vaccine manufacturing for the US market. Mitch Johnson, executive director of the Influenza Franchise for GSK, told the crowd that GSK is “committed to working with the government, public health agencies and healthcare providers to raise awareness surrounding the importance of flu vaccination.”
Lost in Mr. Nowak’s seventeen-slide presentation that day was the acknowledgment that some of the messaging Mr. Nowak was encouraging, and that GSK would later sponsor, looked a lot like lying. Just nine months after Mr. Nowak’s presentation, in an article published in the British Medical Journal (BMJ), Dr. Peter Doshi asked (and answered) a question that put Mr. Nowak’s recommendations under intense scrutiny. Dr. Doshi’s article, “Are US flu death figures more PR than science?” explained that the CDC’s claims of thirty-six thousand annual deaths from flu were “surely exaggerated” and that “until corrected and until unbiased statistics are developed, the chances for sound discussion and public health policy are limited.” In an unusually tough critique, Dr. Doshi (who today serves as editor of the BMJ) even called Mr. Nowak out by name and cited his seven-step recipe as proof of the willingness of the CDC to cite figures and outcomes that science can’t support, all in the name of getting more people vaccinated:
At the 2004 “National Influenza Vaccine Summit,” co-sponsored by CDC and the American Medical Association, Glen Nowak, associate director for communications at the NIP, spoke on using the media to boost demand for the vaccine. One step of a “Seven-Step ‘Recipe’ for Generating Interest in, and Demand for, Flu (or any other) Vaccination” occurs when “medical experts and public health authorities publicly . . . state concern and alarm (and predict dire outcomes)— and urge influenza vaccination.” Another step entails “continued reports . . . that influenza is causing severe illness and/or affecting lots of people, helping foster the perception that many people are susceptible to a bad case of influenza.”
Preceding the summit, demand had been low early into the 2003 flu season. “At that point, the manufacturers were telling us that they weren’t receiving a lot of orders for vaccine for use in November or even December,” recalled Dr Nowak on National Public Radio. “It really did look like we needed to do something to encourage people to get a flu shot.”
A year after Dr. Doshi’s critique, in 2006 Dr. Tom Jefferson of the highly esteemed and independent Cochrane Collaboration issued a blistering report about the flu vaccine, again in the BMJ. Cochrane’s goal as an organization is to provide consumers with “health information that is free from commercial sponsorship and other conflicts of interest,” and Dr. Jefferson’s article, “Influenza vaccination: policy versus evidence,” not only supported Dr. Doshi’s arguments but also challenged the entirety of Mr. Nowak’s messaging (and therefore the CDC’s).
Dr. Jefferson found a “large gap between policy and what the data tell us” and “a gross overestimation of the impact of influenza” and also felt that “the optimistic and confident tone of some predictions of viral circulation and of the impact of inactivated vaccines, which are at odds with the evidence, is striking.” Said differently, he was astonished by how much public health officials were lying, and they urged that a “re-evaluation [of the entire use of flu vaccine] should be urgently undertaken.” It’s rare to see a scientific beat down administered in such striking tones, but neither Dr. Doshi nor Dr. Jefferson held back in their critique that the evidence supporting the flu vaccine recommendations was grossly inadequate.
Dr. Doshi, by now a postdoctoral fellow at Johns Hopkins, took another swing at the flu vaccine in 2013. His essay (once again in the BMJ), “Influenza: marketing vaccine by marketing disease,” should make the CEO of Walgreens, Rite Aid, and any of the other drug stores pushing flu shots every winter season blush with embarrassment. His words were incisive:
Promotion of influenza vaccines is one of the most visible and aggressive public health policies today. Twenty years ago, in 1990, 32 million doses of influenza vaccine were available in the United States. Today around 135 million doses of influenza vaccine annually enter the US market, with vaccinations administered in drug stores, supermarkets—even some drive-throughs. This enormous growth has not been fueled by popular demand but instead by a public health campaign that delivers a straightforward, who-in-their-right-mind-could-possibly-disagree message: influenza is a serious disease, we are all at risk of complications from influenza, the flu shot is virtually risk free, and vaccination saves lives. Through this lens, the lack of influenza vaccine availability for all 315 million US citizens seems to border on the unethical. Yet across the country, mandatory influenza vaccination policies have cropped up, particularly in healthcare facilities, precisely because not everyone wants the vaccination, and compulsion appears the only way to achieve high vaccination rates. Closer examination of influenza vaccine policies shows that although proponents employ the rhetoric of science, the studies underlying the policy are often of low quality, and do not substantiate officials’ claims. The vaccine might be less beneficial and less safe than has been claimed, and the threat of influenza appears overstated.
A reasonable question to ask if you read Dr. Doshi’s essay from start to finish would be, “How does the flu vaccine survive such pointed criticism?” Yet look around today, and nothing has changed. The “36,000 flu deaths per year” unsupportable statistic is still routinely cited, and marketing for the flu shot remains driven by doctors and public health officials predicting dire outcomes that never come to pass, with much of the marketing funded by vaccine makers, who have now combined their marketing message with Covid shots. Head over to the CDC’s website in the fall and winter, and you’ll be greeted with encouragement to get your flu vaccine today, to “protect” both you and your family. When it comes to the flu vaccine, or really any vaccine, the CDC serves as both judge and jury. There is no check, there is no balance. There’s one agency. Many CDC employees end up on the payroll of Big Pharma, like Dr. Julie Gerberding, who parlayed her position as head of the CDC into president of Merck’s vaccine division.
In late 2017 Science Magazine further exposed the limitations and false assumptions behind the flu vaccine in an article titled, “Why flu vaccines so often fail.” It turns out the reason is more complicated than the oft-repeated claim that it’s hard to guess what the primary strain of flu will be next season:
For many decades, researchers believed the flu vaccine offered solid protection if it was a good match to the circulating strains; studies from the 1940s through the 1960s routinely showed an efficacy of 70% to 90%. But those studies relied on a misleading methodology. Without a simple way to detect the virus in the blood, researchers measured antibody levels, looking for a spike that occurs after infection. Then in the 1990s, sensitive polymerase chain reaction tests enabled researchers to actually measure viral levels, and they told a different story. It turned out that some people who did not have the big antibody spike after exposure—and were therefore counted as a vaccine success—actually did show a jump in viral levels, signaling infection. Earlier assessments had exaggerated vaccine efficacy. What’s more, efficacy was sometimes low even when the vaccine and circulating strains appeared well matched.
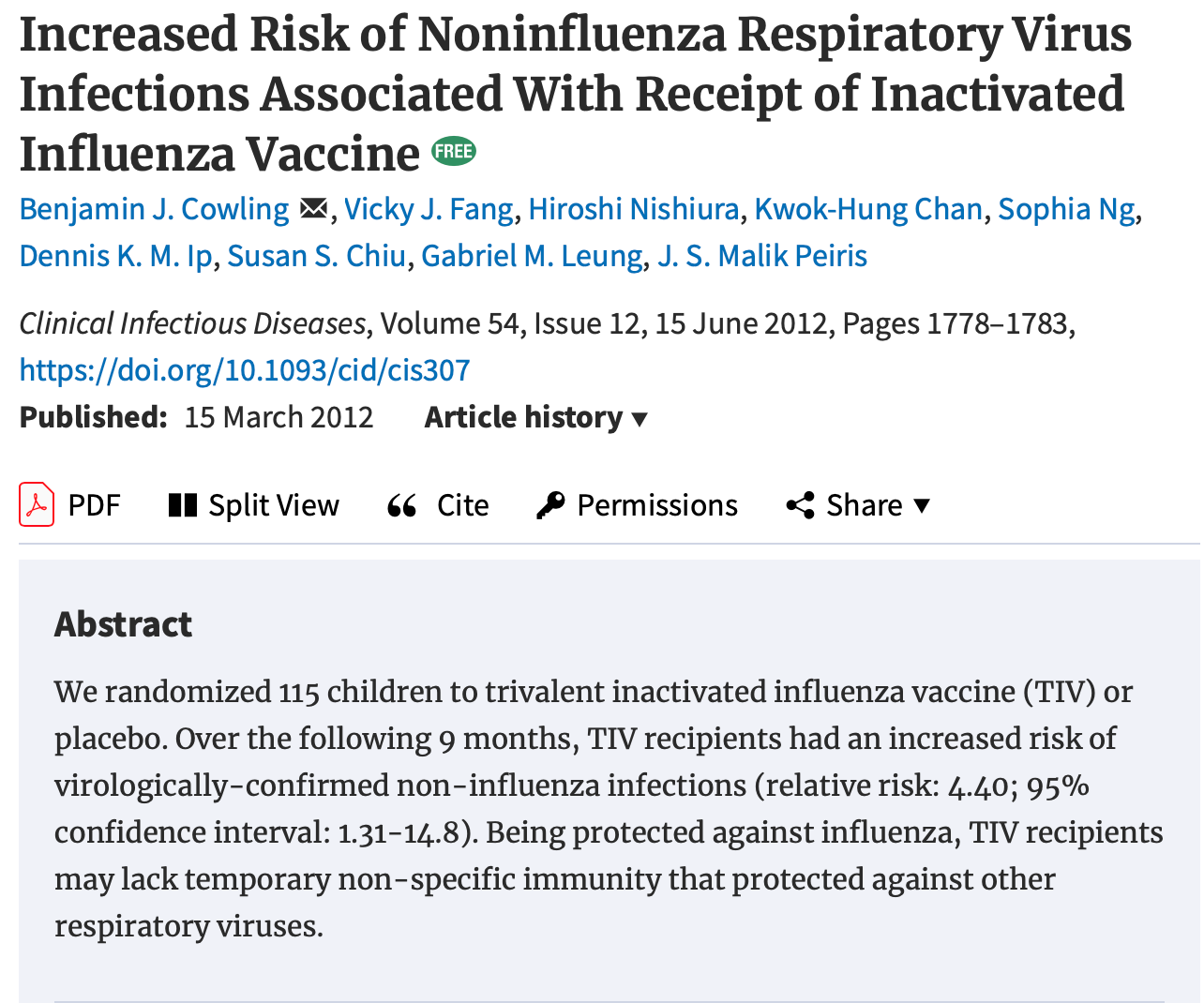
In 2012 the news got worse for the flu vaccine with the publication of a study in Clinical Infectious Diseases that found that children who had received the flu vaccine didn’t have a lower risk of getting the flu, but they had a more than four times higher risk of getting other respiratory infections, causing the researchers to conclude that “the protection against influenza virus infection conferred by TIV [flu vaccine] was offset by an increased risk of other respiratory virus infection,” which they attributed to the flu vaccine’s “viral interference” with the natural immune system.
How come the public is never told about all this new information? We can learn a lot from the unwillingness of public health officials to amend their story when called out in esteemed medical journals. From Mr. Nowak’s “recipe” we know that public health officials are willing to exaggerate, spin, and lie when appropriate as a matter of policy.
Vaccines Didn’t Save Humanity
Hiding in plain sight and published in the AAP’s own journal, Pediatrics, is a study from 2000 by public health scientists from both the CDC and the Johns Hopkins School of Public Health that singularly refutes the oft-told lie that vaccines saved humanity. As anyone who studies public health can tell you, clean water, sanitation, plumbing, refrigeration, and proper food handling are far more important to reducing the spread of infectious disease, and it was the gains in these standards of living in the United States that lead to a dramatic drop in death from infectious disease. How big a drop? In the study, “Annual Summary of Vital Statistics: Trends in the Health of Americans During the 20th Century,” the scientists explain that “vaccination does not account for the impressive declines in mortality seen in the first half of the century…Nearly 90% of the decline in infectious disease mortality among US children occurred before 1940, when few antibiotics or vaccine were available.
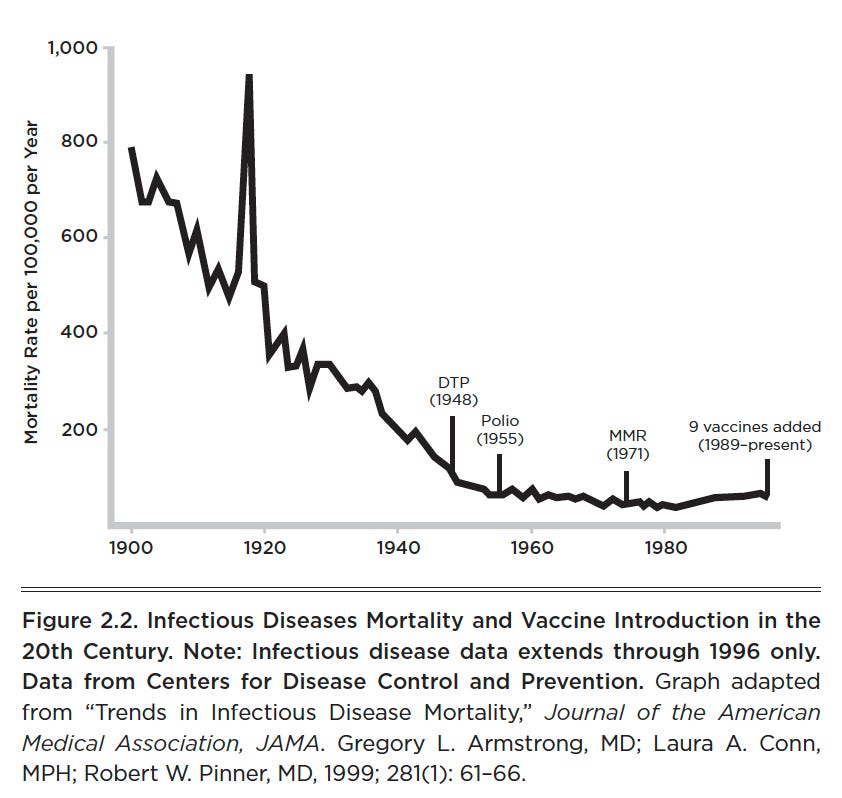
What did contribute to a massive decline in child mortality from the early 1900s to the end of the twentieth century? The study cites a number of things, including local health departments being created in every state, water treatment, food safety, waste disposal, decreased crowding in urban housing, and “public education about hygienic practices.” What’s particularly odd is that many other infectious diseases also declined precipitously, despite the fact that no vaccine ever existed for them—how can both be true? As Dr. Jayne Donegan explains:
It was a received “article of faith” for me and my contemporaries, that vaccination was the single most useful health intervention that had ever been introduced. . . . I was taught that vaccines were the reason children and adults stopped dying from diseases for which there are vaccines. . . . We were told that other diseases, such as scarlet fever, rheumatic fever, typhus, typhoid, cholera, and so on, for which there were no vaccines at the time, diminished both in incidence and mortality due to better social conditions. You would think that some of us would have asked, “But if deaths from these diseases decreased due to improved social condition, why mightn’t the ones for which there are vaccines also have decreased at the same time for the same reason?”
By the way, I found this topic so fascinating, I wrote an article about it:

Smallpox and John Thomas Biggs
Well ahead of his time, Englishman John Thomas Biggs was the sanitary engineer for his town of Leicester and had to actively respond to outbreaks of smallpox. He quickly learned that the public health outcomes from sanitation vastly outweighed the impact of vaccination (where he saw dramatic vaccine injury and ineffectiveness). He wrote a definitive work in 1912, Leicester: Sanitation versus Vaccination.More than one hundred years ago, Mr. Biggs had discovered what the CDC reaffirmed in 2000: Nothing protects from infectious disease like proper sanitation. He explained:
Leicester has furnished, both by precept and example, irrefutable proof of the capability and influence of Sanitation, not only in combating and controlling, but also in practically banishing infectious diseases from its midst. . . . A town newly planned on the most up-to-date principles of space and air, and adopting the “Leicester Method” of Sanitation, could bid defiance not to small-pox only, but to other infectious, if not to nearly all zymotic, diseases.
Dr. Andrew Weil, the oft-quoted celebrity doctor, reenforces the point, explaining that “medicine has taken credit it does not deserve for some advances in health. Most people believe that victory over the infectious diseases of the last century came with the invention of immunizations. In fact, cholera, typhoid, tetanus, diphtheria, and whooping cough, and the others were in decline before vaccines for them became available — the result of better methods of sanitation, sewage disposal, and distribution of food and water.”
Vaccines didn’t save humanity. Improvement in sanitation and standards of living really did. Did vaccines contribute to a small decrease of certain acute illnesses? Yes, but their relative benefit is often exaggerated to an extreme. Consider this: In late 2017 it was reported that Emory University scientists were developing a common cold vaccine. Professor Martin Moore bragged that his research “takes 50 strains of the common cold and puts it into one shot” and that the monkeys who served as test subjects “responded very well.” You should expect to see this vaccine at your pediatrician’s office in the next five years, which will likely be rolled out soon after the stories start to appear in the media about the common cold causing childhood deaths.
The Myth of Herd Immunity? They Forgot to Count Adults
If you still need more convincing that public health officials and vaccine makers will mislead the public, consider the fable of “herd immunity,” the oft-cited reason that everyone needs to be vaccinated. If most people (“the herd”) are vaccinated against an illness, the story goes, then the herd is protected from that disease. In many cases pediatricians and talking heads will get very specific about herd immunity, citing important-sounding statistics that say vaccination rates on certain diseases must stay above a certain percentage of people to have herd immunity. Drop below that threshold? It’s a recipe for disaster. When there was an “epidemic” of measles (it wasn’t actually an epidemic, just a minor and typical outbreak) at Disneyland a few years ago, experts were quoted on TV saying the herd immunity threshold for measles vaccine was 95 percent, meaning 95 percent of the population needed to be vaccinated against measles to prevent “epidemics.”
Perhaps no one has beaten the herd immunity drum more loudly than California State Senator Richard Pan, the author and sponsor of SB277, a bill that made California the third state in the union (Mississippi and West Virginia are the other two) to make vaccinations mandatory for children’s school attendance. In fact, he used the Disneyland measles outbreak as the reason his bill needed to be passed. In a recent missive to his constituents, Senator Pan noted that his 2015 bill was raising kindergarten vaccination rates and bragged, “This success is a first step toward reducing the number of unimmunized people putting our families at-risk for preventable diseases, thereby restoring community immunity throughout our state in the coming years.”
Let’s look at Senator Pan’s words carefully. “Restoring community immunity” has several implications. Firstly, it implies that California had somehow “lost” community immunity (which is a nonscientific synonym for herd immunity) at some point. Secondly, “restoring” community immunity implies that until vaccination rates hit a certain threshold, grave risks will be present—restoration of safety is a top priority! The absurdity of Senator Pan’s convictions about the importance of herd immunity and of hitting certain vaccination targets is that the United States has never been close to achieving herd immunity for any vaccine-preventable disease for two simple reasons: (1) The overwhelming majority of adults in the United States are not up to date on their vaccines, and (2) The efficacy of vaccines to prevent disease wanes over time, meaning protection from a vaccine “wears off,” typically in ten years or less. (It’s called “protection waning.”)
Slovak scientists realize MMR protection wears off fast
A recent study in 2023 provided details for how quickly immunity was lost from the vaccine considered to provide the most long-term protection: MMR> The scientists discovered that most people lost measles protection from the vaccine in 10 years, meaning most people over the age of 15 have no vaccine-derived protection to measles. The scientists concluded: “from a long-term perspective, waning immunity may have a significant impact on the population’s susceptibility to measles, and it is important to explore this phenomenon.”
To put this in perspective, there are roughly 150 million adults in the United States walking around with no vaccine-provided protection from many diseases that we are supposed to have met herd immunity thresholds for. The CDC surveys adults every year, so it’s easy enough to find vaccination coverage rates. Here are just a few: hepatitis A (9 percent), hepatitis B (24.5 percent), pneumococcal (20.4 percent), and influenza (43.2 percent). These adults work in schools (where they don’t have the same immunization requirements as children), work in restaurants, work in stores, and are in every community, which means we are nowhere close to herd immunity and never have been. In fact, I don’t think most adults even realize the CDC maintains an adult immunization schedule. When people like Senator Pan pat themselves on the back for protecting society by reestablishing herd immunity, it has no basis in fact. With so many people unvaccinated, where are all the crippling epidemics?
In an article in the congressional newspaper The Hill titled, “If only half of America is properly vaccinated, where are the epidemics?” written by Gretchen DuBeau, the executive director of the Alliance for Natural Health, she explains this logic gap, writing:
While herd immunity may not exist, herd mentality most definitely does. Health authorities, media commentators, and schools and their parent–teacher associations waste no opportunity in perpetuating this myth. Proponents have done such a thorough job of convincing the public that a parent who questions it is treated like someone who thinks the earth is flat or believes climate change is a conspiracy. On the contrary: an unprejudiced view of the science about vaccines, and an examination of history, clearly show that the herd immunity theory is—and always has been—flawed.
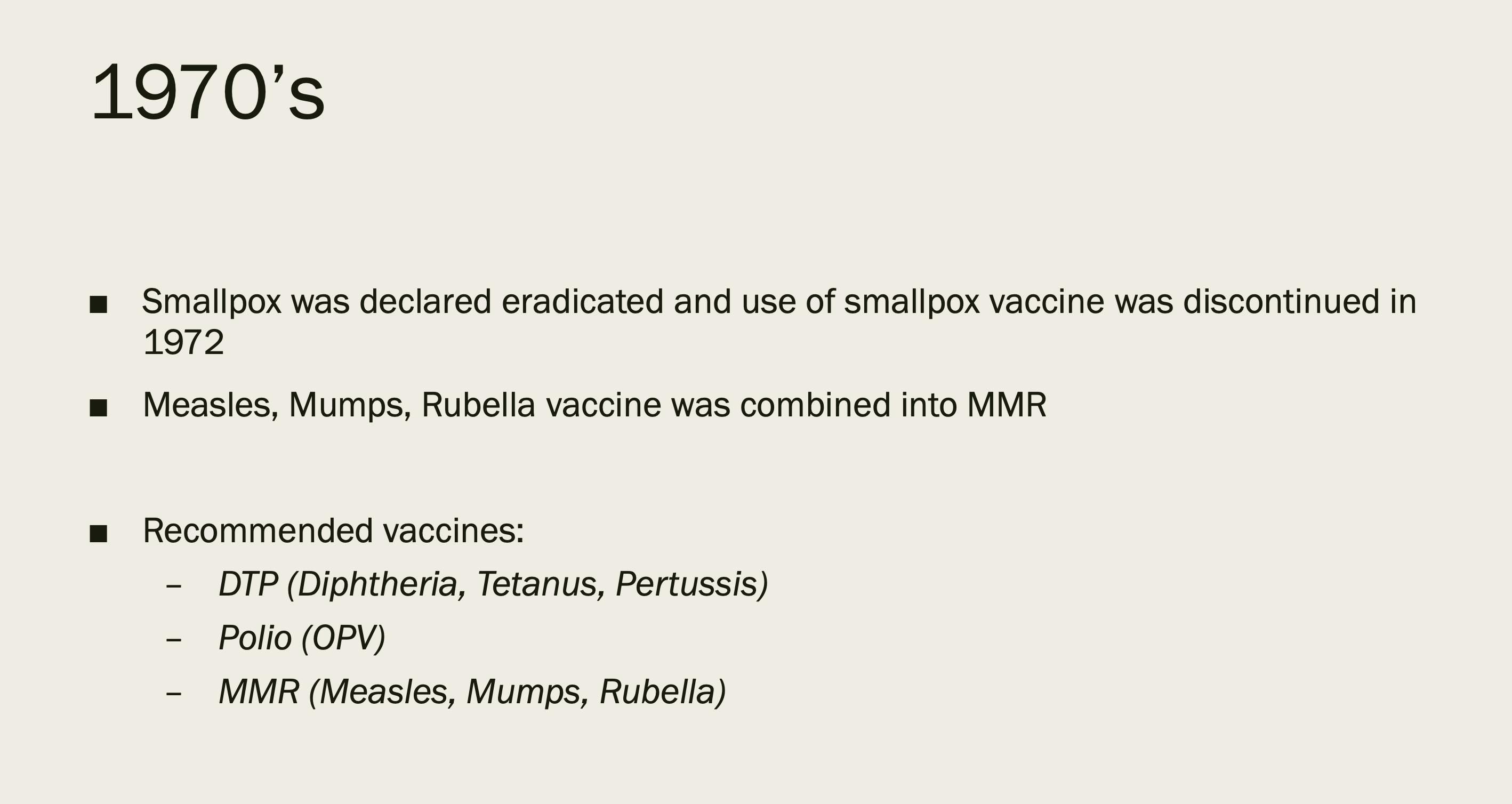
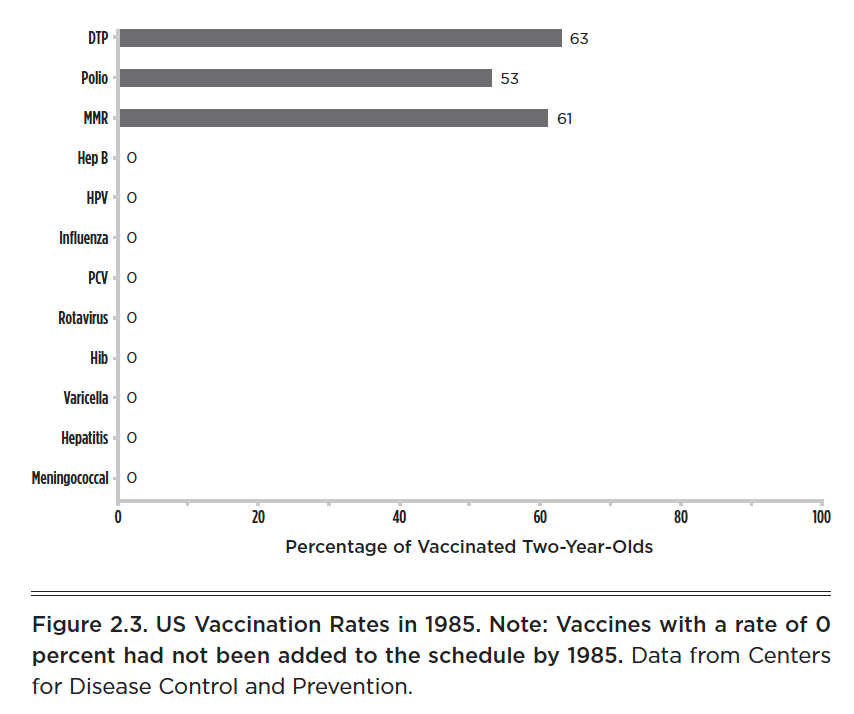
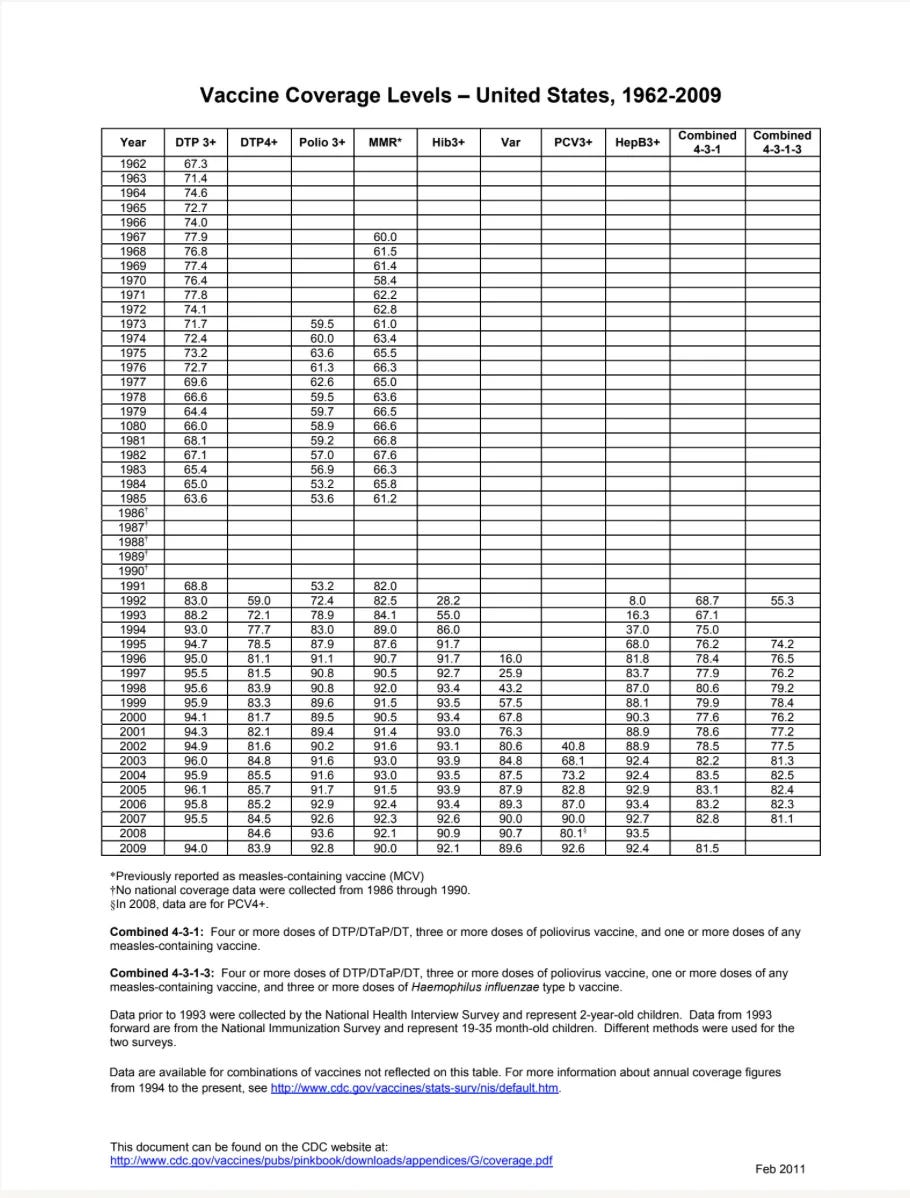
Vaccination rates among American children for the three primary vaccines given in the 1960s and 1970s were far lower than today’s vaccination rates. For example, in 1973 the first year the CDC tracked polio vaccination rates, the vaccination rates for DTP (diphtheria, tetanus, and pertussis or whooping cough), polio, and MMR were 72 percent, 59 percent, and 61 percent, respectively. In 1985 those numbers were 63 percent, 53 percent, and 61 percent (see image). Much as the question is asked of adults today, where were all the childhood epidemics in 1973 and 1985 with such “low” vaccination rates? They didn’t exist.
Politicians stand up in front of their colleagues, pound the table, and advocate passing mandatory vaccination laws to “preserve herd immunity.” Pediatricians get on TV and explain how critical it is that we all “maintain herd immunity.”
The notion of herd immunity is nonsense. The truth is out there for any parent willing to look at the facts.
Vaccine Makers Are Indemnified
On October 20, 1986, the Los Angeles Times ran a story regarding a controversial bill making its way through Congress. The headline shouted, “Vaccine Injury Fund Bill Approved but Faces Veto.” The story went on to explain the divisive nature of the bill, intended to shield vaccine makers from liability if their product caused harm, and the Reagan administration was speaking out to express their opposition:

In a strongly worded letter to House Speaker Tip O’Neill, the then secretary of the Department of Health and Human Services, Otis R. Bowen said, “The bill is likely to do little to assure the vaccine supply or to improve our childhood immunization efforts.” Assistant Attorney General John R. Bolton, writing to the head of the House Judiciary Committee on behalf of the Department of Justice, said the White House opposed the legislation because it was creating, “a major new entitlement program for which no legitimate need has been demonstrated.” President Reagan was troubled by the vaccine compensation bill and was quoted as saying, “Although the goal of compensating those persons is a worthy one, the program has . . . serious deficiencies.”
The Reagan administration seemed to be particularly concerned with two issues: who was going to pay for the compensation required for vaccine injury and the precedent of the federal government indemnifying private companies from liability. As the New York Times reported, “The program would be ‘administered not by the executive branch, but by the Federal judiciary,’ Mr. Reagan said, calling it an ‘unprecedented arrangement’ that was inconsistent with the constitutional requirement for separation of powers among the branches of the Federal Government.’”
The National Childhood Vaccine Injury Act was actually part of a larger bill, the Omnibus Health Bill (S. 1744), that was introduced in the waning days of the Ninety-Ninth Congress in late 1986. Leading a four-year effort to pass the controversial legislation on vaccine liability was a congressman from California, Henry Waxman. Waxman’s bill was supported by vaccine manufacturers, who were lobbying hard on its behalf, and the American Academy of Pediatrics.
To be fair, like many pieces of legislation, the bill had some reasonable intentions. Unbeknownst to most parents today, an older version of the DPT shot was causing severe brain damage in many children, and parental lawsuits against vaccine makers were mounting. There was genuine fear that pharmaceutical companies might get out of the vaccine business altogether, because the risks were too high (not very comforting). And the bill proposed the establishment of VAERS—today’s Vaccine Adverse Event Reporting System—which beat the nonexistent safety monitoring system in place at the time.
With only days to go before the congressional recess, the bill’s passage was up in the air, with the White House declaring plans to veto the entire omnibus package, due almost exclusively to the provisions in the National Childhood Vaccine Injury Act. Congressman Waxman, the bill’s author, was unyielding and worked the press to his advantage in the final days, declaring:
This bill is the first step to taking care of children hurt in the process of protecting society from epidemics, and to ensure an adequate supply of vaccines. . . . If the President vetoes it, he will leave these children to fend for themselves and leave the country with risks or shortages or skyrocketing prices. . . . If he vetoes it, I hope he has some emergency plans to start making vaccines himself because the manufacturers tell us they may very well stop.
Worried by the threat of losing the entire manufacturing base of vaccine makers coming from Henry Waxman and the AAP, Ronald Reagan made the bill law on November 15, 1986, “with mixed feelings” and “serious reservations.” He gave vaccine makers an early holiday gift when it came to vaccines, as the new law made clear:
No vaccine manufacturer shall be liable in a civil action for damages arising from a vaccine-related injury or death associated with the administration of a vaccine after October 1, 1988, if the injury or death resulted from side effects that were unavoidable even though the vaccine was properly prepared and was accompanied by proper directions and warnings.
What happened next should surprise no one who understands how capitalism works. The same industry that brought you Vioxx, thalidomide, fen-phen, Prozac, and the opioid epidemic had just had product liability removed and handed over to a newly established “vaccine court” that would be funded with a surtax on every vaccine purchased (yes, Americans fund the vaccine injury compensation program when they pay for a vaccine for themselves or their child) and ultimately managed and backstopped by the federal government. Remember, when this bill was passed in late 1986, it was viewed as a way to keep vaccine makers in the vaccine business. I’m not sure anyone (except perhaps pharmaceutical company executives and their lobbyists) could have predicted how vastly things would change. Consider the following:
In 1962 a child following the CDC’s recommended schedule would have received three vaccines by age five.
In 1983 a child following the CDC’s recommended schedule would have received ten vaccines by age five.
In 2018 a child following the CDC’s recommended schedule received thirty-eight vaccines by age five, nearly quadruple what a child received in the 1980s and more than twelve times what a child received in the 1960s.
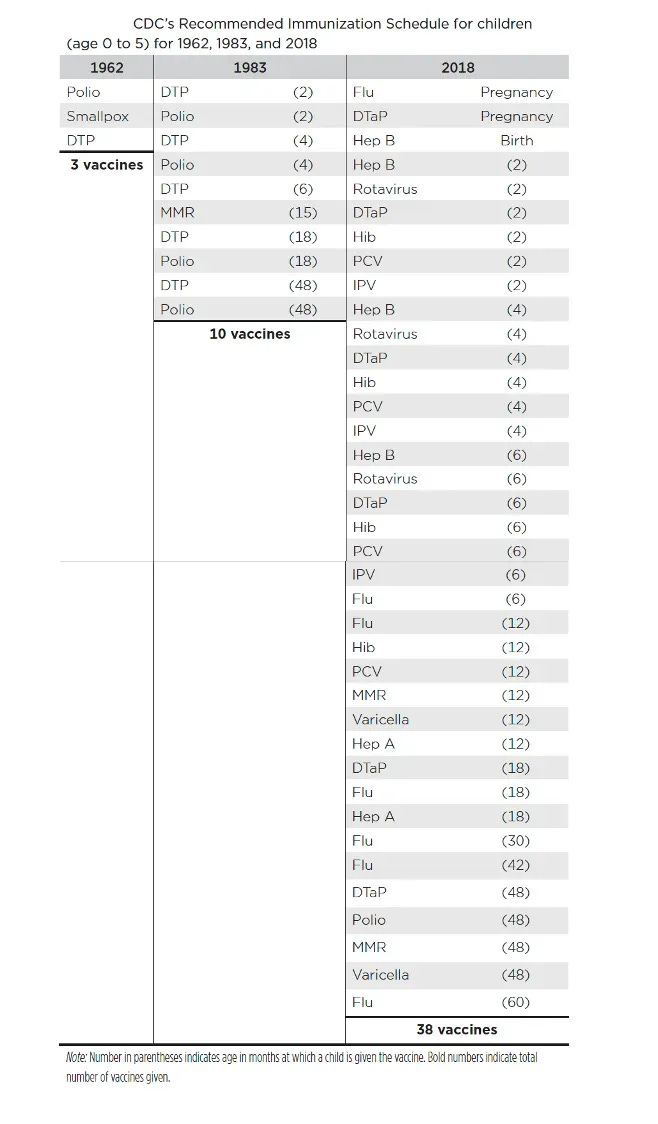
When I was a child in the 1980s, there were just three vaccines that children received: DTP, polio, and MMR (administered several times to “boost” immunity). Today, influenza (Flu), hepatitis B, hepatitis A, haemophilus influenzae type B (Hib), pneumococcal conjugate (PCV), rotavirus, meningitis, and varicella (chickenpox) vaccines have all been added to the childhood schedule (and been given multiple times through booster shots). When someone asks you if your child is “fully vaccinated,” perhaps the right reply is, “Based on which decade?” It’s worth noting that children were not “dying in the streets” during the 1980s, when we gave far fewer vaccines (and had one in ten thousand children with autism).
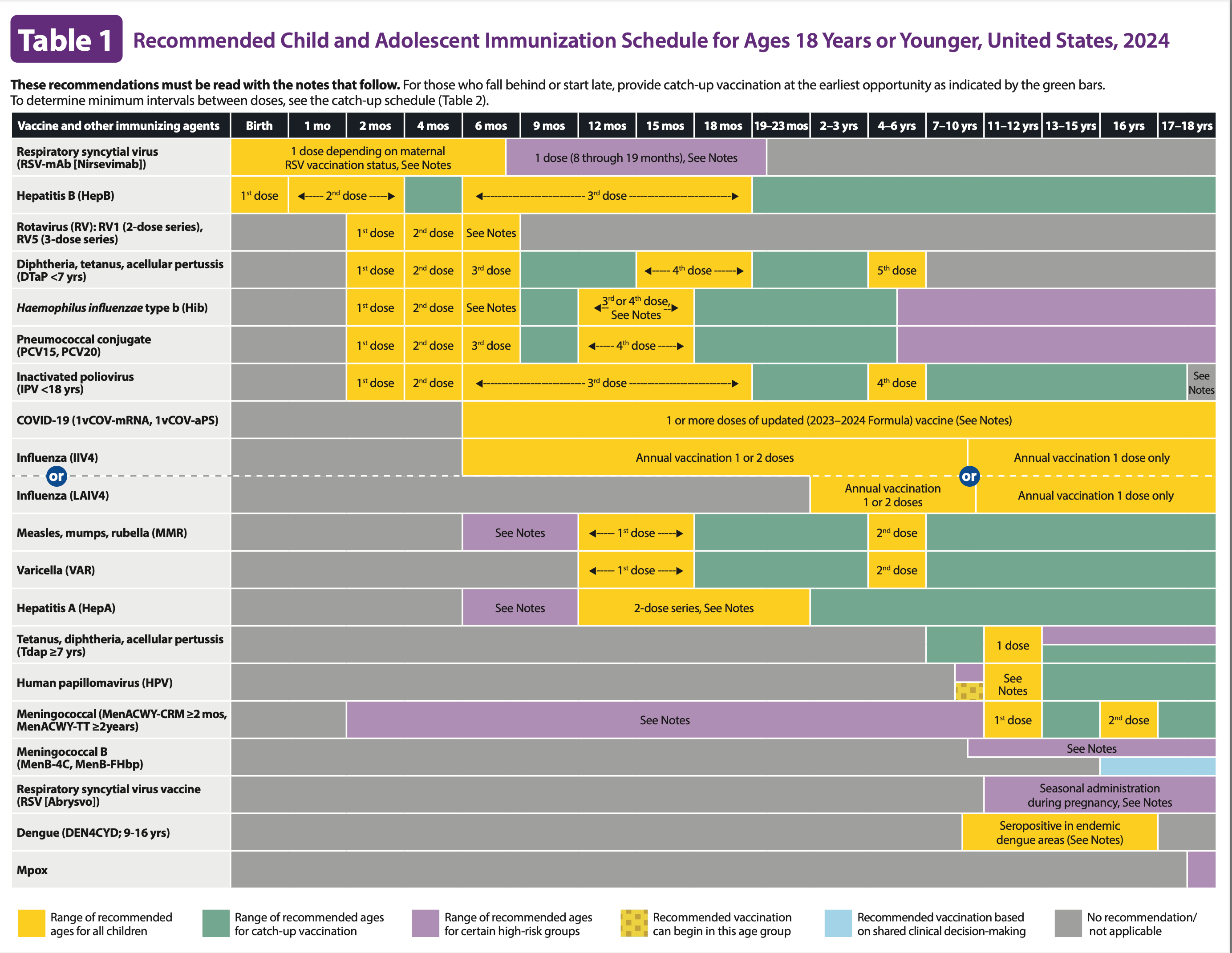
Let me pause for a moment and draw your attention to the words “recommended schedule.” If as a parent you are wondering about what vaccinations your child will receive at her next “well baby” visit, you might visit the CDC’s website and find the “recommended schedule.” Be aware that this schedule is not “recommended” to parents, as if you have agency (though the CDC wants you to believe you do). This schedule is recommended to the AAP, which instantly adopts it, and pediatricians, who often receive bonuses for full vaccine compliance in their practice. For parents it is a de facto mandated schedule because in most states your child can’t attend school without being vaccinated. While you might seek out an exemption—religious, philosophical, medical—these are getting harder and harder to come by. In fact, there is a movement by many state legislatures to remove vaccine exemptions altogether, as California did in 2015 with the passage of SB 277 (becoming the third state with only a medical exemption, followed soon after by New York and Connecticut).
As of today, the vaccine court created in 1986 has paid out more than $3.7 billion for vaccine injury claims—remember, funded by American taxpayers. The majority of those claims are filed by the families of vaccine-injured children. Meanwhile, the market for vaccines is expected to be worth $60 billion in 2020,up from $170 million in the early 1980s, just as the 1986 act was put in place. As the New York Times reported in 2014, “Once a loss leader for manufacturers, because they are often more expensive to produce than conventional drugs, vaccines now can be very profitable. . . . Since 1986, they have pushed up the average cost to fully vaccinate a child with private insurance to the age of 18 to $2,192 from $100, according to data from the Centers for Disease Control and Prevention.”
It’s hard to believe. The one thing that could slow the party down on the way to sixty billion dollars is consumer doubt. If parents don’t question vaccines, just as my wife Lisa and I did not, the juggernaut steams forward to more profits. But if parents begin to doubt vaccine safety, Big Pharma could be looking at a titanic loss. That’s where autism comes into play. At a rate of one in thirty-six, this is not an acceptable trade-off. It’s not that hard to imagine why there is so much suppression of the truth, and such vicious fighting.
Other Countries Give Far Fewer Vaccines
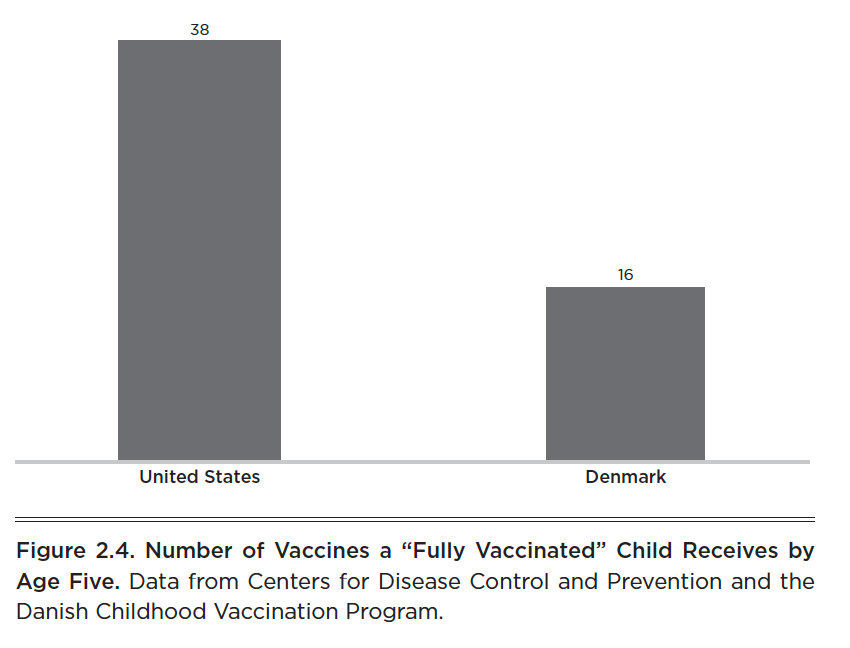
Even the definition of “vaccinated” is hard to pin down. Not only did being vaccinated mean something very different twenty years ago, being vaccinated today varies depending on where you are born in the world. Take, for example, the vaccination schedule of Denmark, which is managed and monitored by the Danish Health and Medicines Authority. It provides parents with a scheduled childhood vaccination program, similar to that of the United States, but missing from the Danish schedule are the following five vaccines that American children get: hepatitis B, hepatitis A, influenza (flu), rotavirus, and varicella (chickenpox).
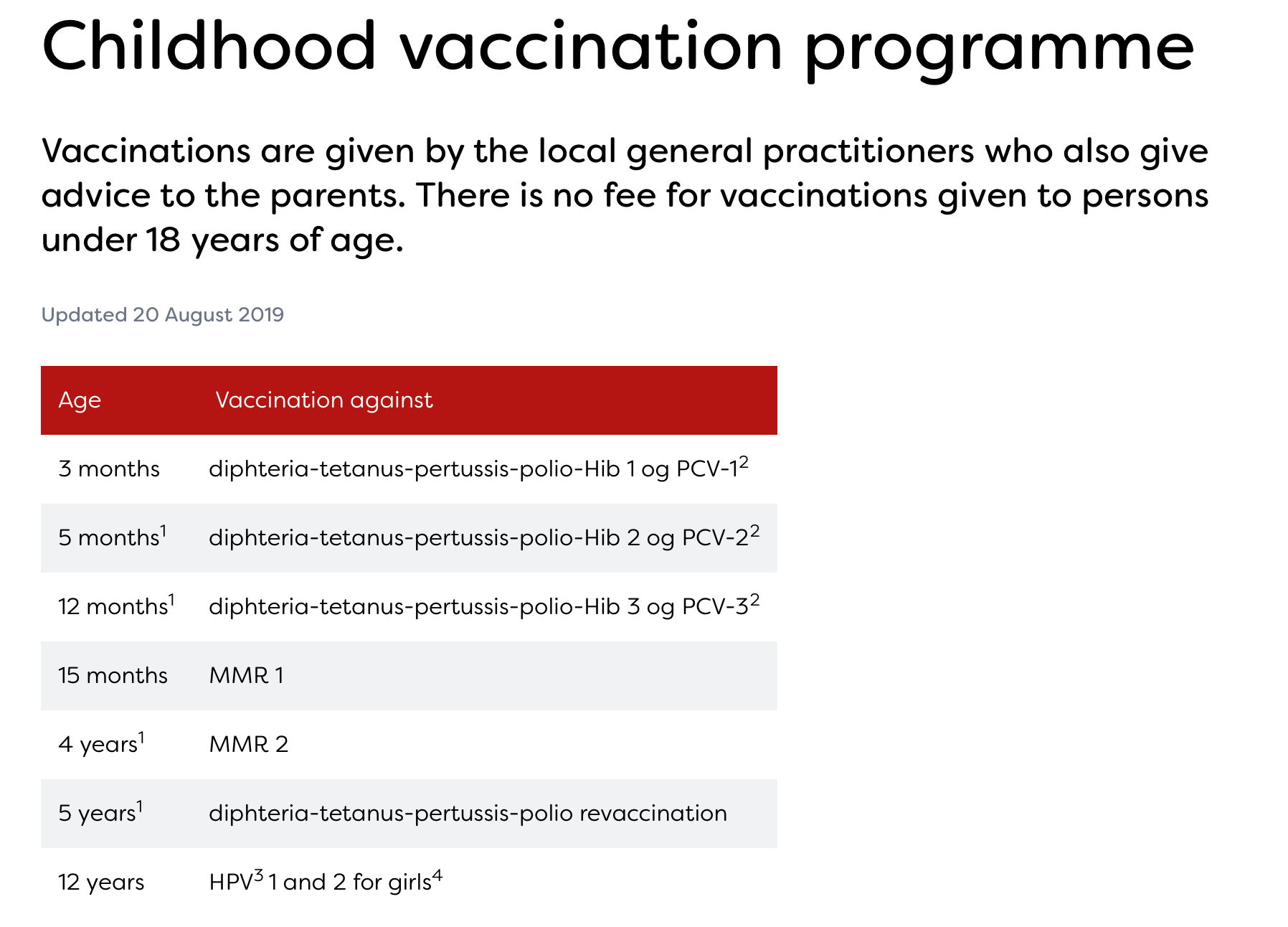
A “fully vaccinated” American child and a fully vaccinated Danish child are not the same. A Danish child gets far fewer vaccines (sixteen total vaccines in Denmark versus thirty-eight in the United States). If these vaccines are vitally important, why would a country that serves as an entry point for many to travel to Europe exclude the vaccinations on the American schedule? Hepatitis B vaccine is only given in most European countries to the offspring of mothers who have hepatitis B themselves. Most European countries do not routinely give hepatitis A, rotavirus, varicella (chickenpox), or the flu shot.
Digging a little deeper, we find that the United Kingdom doesn’t give children the chickenpox vaccine. In the UK the National Health Service (NHS) manages the vaccine program, and they explain why they have chosen not to give the varicella (chickenpox) vaccine to children:
The chickenpox vaccine is not part of the routine UK childhood vaccination programme because chickenpox is usually a mild illness, particularly in children. There’s also a worry that introducing chickenpox vaccination for all children could increase the risk of chickenpox and shingles in adults.
In England chicken pox is not a recommended vaccine, but a parent in the United States who chooses to avoid the chickenpox vaccine might be chided by her pediatrician for “undervaccinating” her child or have trouble enrolling that child in daycare or school. Welcome to the land of vaccination confusion.
No Vaccines for Many Infectious Diseases
I live in Oregon. Like every state, we have a state health department. In our case it’s the Oregon Health Authority, or OHA. In order to manage the monitoring of infectious disease, the state has laws about how quickly a health-care provider must report the presence of certain infectious diseases in a patient to the OHA. Diseases are classified into three categories: report immediately, report within 24 hours, and report within one working day—it’s a ranking system for how concerned the OHA is about various infectious diseases.
There are sixty-seven total diseases that are “reportable” in my state. Of those sixty-seven, we have vaccines for only ten. The other fifty-seven reportable diseases have no vaccine available. Of the seventeen diseases that require immediate reporting, we vaccinate for four of them, leaving 100 percent of children “unprotected” against the other thirteen diseases!
Vaccines don’t form a protective ring around anyone; our immune system remains our primary defense against disease, at least for the fifty-seven reportable ones here in Oregon for which we have no vaccine. As best-selling author Dr. Bob Sears explains:
A healthy immune system is the key to preventing infectious diseases. We are all exposed to millions of germs every day, and vaccines only cover a tiny fraction of one percent of these germs. So we must rely on our own immune system to fight off most potential infections.
In fact, I’d argue most people’s understanding of what a vaccine does and how it works is cartoonishly simple and goes something like this: You get a perfectly safe vaccine, it boosts your immune system, and then you’re protected from whatever disease you were vaccinated for, perhaps forever. Except no part of that simple explanation is true.
There Will Always Be Outbreaks
Every year there are reported outbreaks of pertussis, mumps, and measles. There’s a simple explanation for this consistency, and it’s not what you think. Put simply: The vaccines don’t work that well. As the Associated Press reported in 2013:
“A government study offers a new theory on why the whooping cough vaccine doesn’t seem to be working as well as expected. The research suggests that while the vaccine may keep people from getting sick, it doesn’t prevent them from spreading whooping cough — also known as pertussis — to others. “It could explain the increase in pertussis that we’re seeing in the U.S.,” said one of the researchers, Tod Merkel of the Food and Drug Administration.
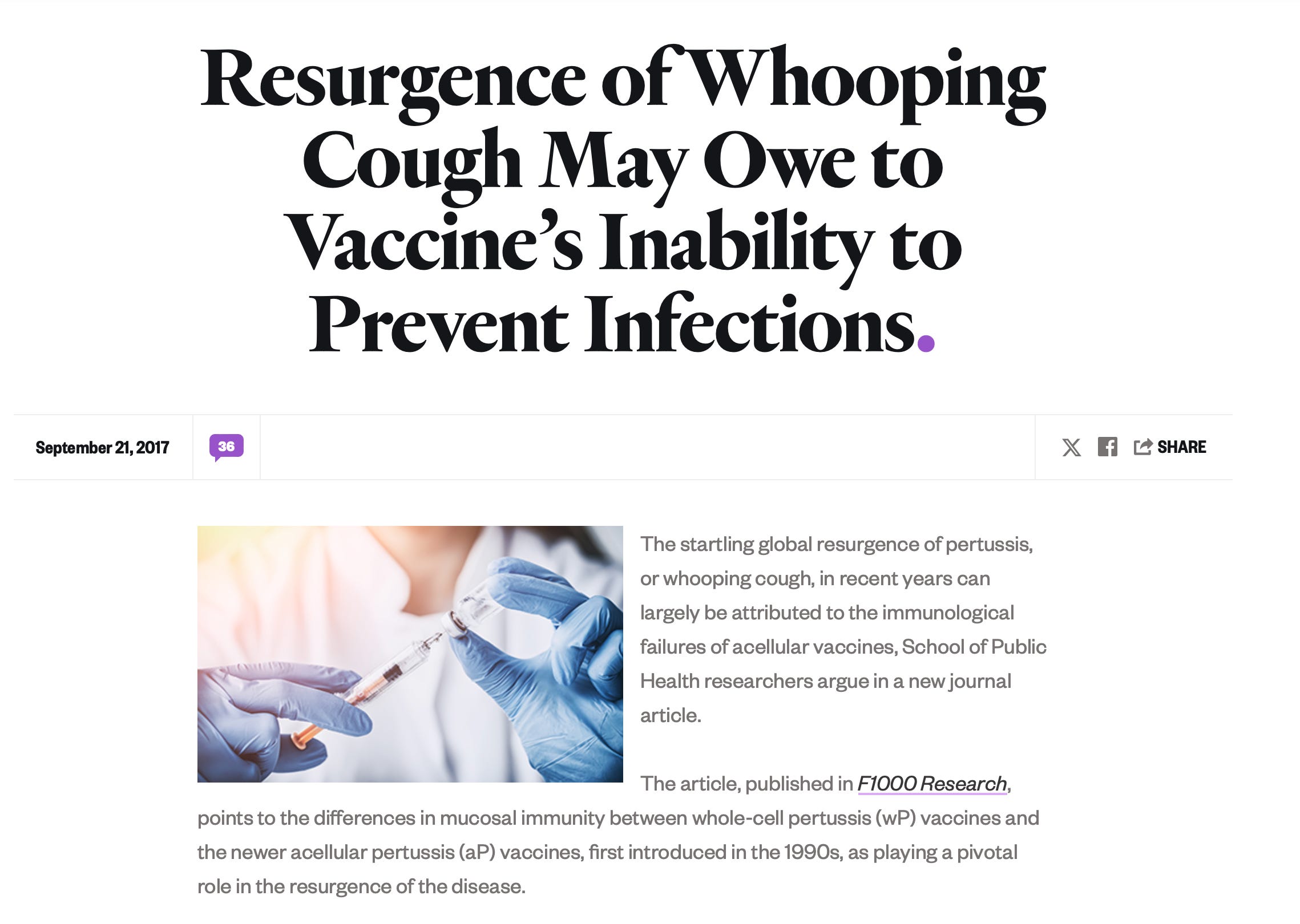
In 2017 public health researchers at Boston University argued that the resurgence of whooping cough cases “can largely be attributed to the immunological failures of acellular vaccines,” as lead researcher Dr. Christopher J. Gill explained
:
This disease is back because we didn’t really understand how our immune defenses against whooping cough worked, and did not understand how the vaccines needed to work to prevent it. Instead we layered assumptions upon assumptions, and now find ourselves in the uncomfortable position of admitting that we may [have] made some crucial errors. This is definitely not where we thought we’d be in 2017.
And the media reporting on measles and other outbreaks rarely explains that the majority of people infected with pertussis or measles or mumps have been vaccinated. There was a mumps outbreak at Harvard University just a few years ago. It turns out “the infected students had all been vaccinated against mumps, as required by law. It’s possible the vaccine didn’t work in some people, or that the virus mutated in ways that made the shot less effective. The mumps vaccine fails to induce immunity in about 12 percent of people who receive it, so mumps outbreaks occur occasionally even in highly vaccinated populations.”
In 2017 the CDC’s own Advisory Committee on Immunization Practices held an October meeting to discuss the issue of vaccine effectiveness, explaining that “research suggests that 10 or more years after the second childhood dose [of mumps], protection against the virus fades enough to help outbreaks take hold.” It’s worth noting there is a whistle-blower lawsuit against Merck in Pennsylvania, the maker of the mumps vaccine, with former Merck employees claiming Merck hid the efficacy data on mumps, because it was showing that the vaccine often didn’t work. The whistle-blowers charged that “the drug maker knew its vaccine was less effective than the purported 95% level, and alleged senior management was aware and also oversaw testing that concealed the actual effectiveness.”
Vaccine Safety Testing Is Inadequate
Vaccines aren’t required to undergo double-blind trials before they are given to babies. When a pharmaceutical company tests vaccines, they don’t have a “control group” receiving a placebo vaccine to see if there is a difference in adverse outcomes from getting a new vaccine. Worse, the safety testing during a new vaccine trial evaluates adverse reactions after participants received a vaccine for somewhere between two and five days. As one example, the only stand-alone polio vaccine in the United States was monitored for only forty-eight hours after administration.That’s it. Autism, which takes time to manifest, would never be captured in these safety trails. In fact, many of the known adverse events from vaccines with names like Guillain-Barré syndrome, chronic inflammatory demyelinating polyneuropathy, and rheumatoid arthritis may take weeks, months, or even years to manifest, so safety testing wouldn’t capture any of them.
As another example, the safety study from Recombivax, one of the most widely used hepatitis B vaccines in the world, and given to many American babies on day one of life, included “434 doses of RECOMBIVAX HB, 5 mcg . . . administered to 147 healthy infants and children (up to 10 years of age) who were monitored for 5 days after each dose.” The entire safety profile for this vaccine, given to millions of children, was based on 147 infants who were monitored for five days. And the infants were not given any other vaccines, despite the fact that at two months, four months, six months, and twelve months of age, babies simultaneously receive at least four other vaccines: rotavirus, DTP, Hib, and PCV. As pediatrician Dr. Harold E. Buttram explains in a letter to the BMJ:
In order to meet the criteria of scientific proof, a vaccine safety study would need to perform before-and-after human studies designed to screen for possible adverse effects on the neurological, immunologic, and hematological systems, comparing vaccinated with unvaccinated subjects, both in sufficient numbers and followed for sufficient periods of time to be meaningful. There have never been any studies of this nature, and apparently none have been attempted. Based on personal observation, it appears that before-and-after testing has been studiously avoided by government health agencies for fear that the results would discourage public confidence in vaccine programs. Until this level of safety testing is done, it is a virtual certainty that many adverse vaccine reactions are taking place unrecognized and will continue to take place. By the same token, until meaningful, objective vaccine safety testings are done, in my opinion the NIH, CDC, FDA can justifiably be accused of negligence in protecting the health and welfare of the American public, especially the children.
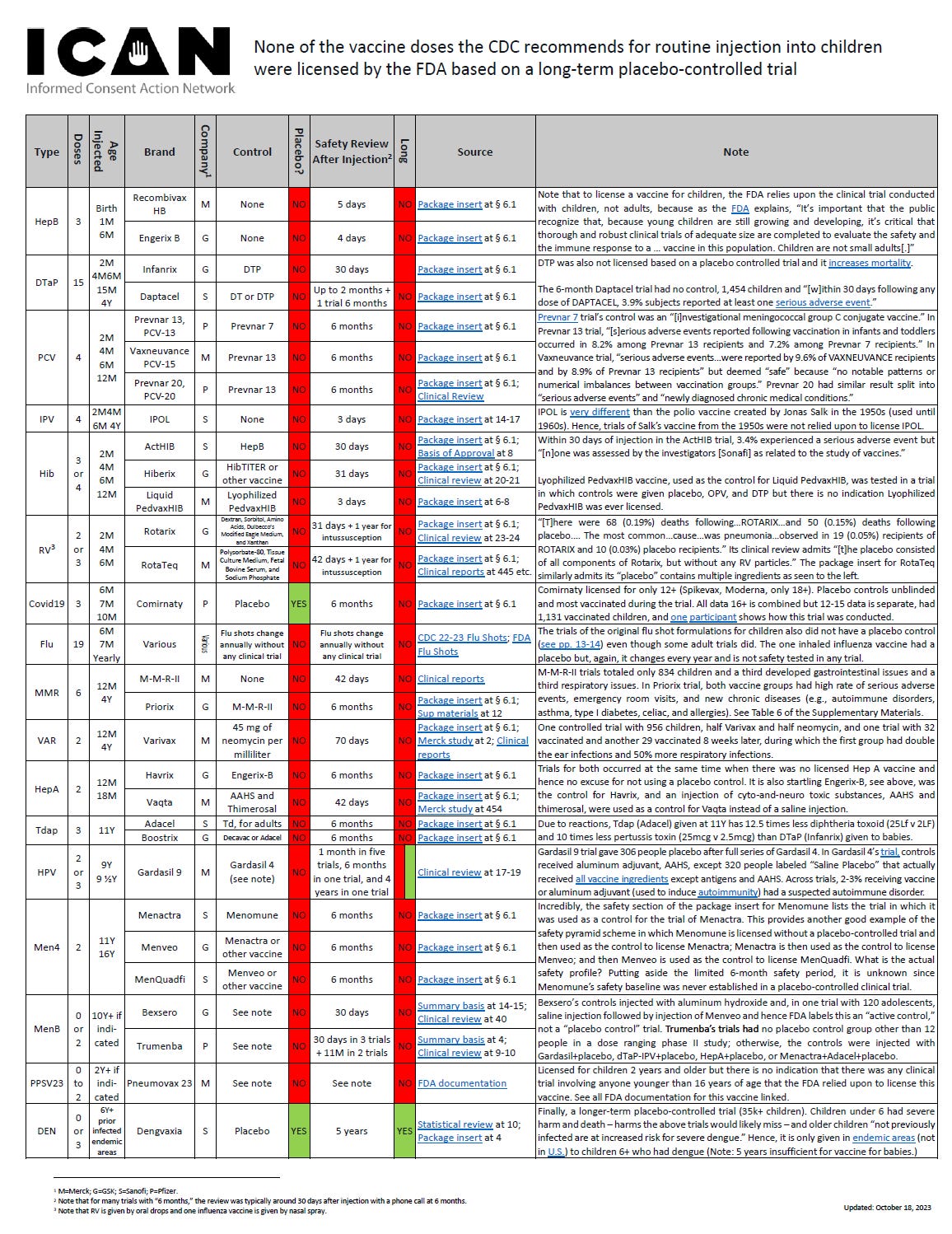
No group has done more to expose this testing inadequacy than the Informed Consent Action Network. They put a comprehensive chart together of the work—or lack thereof—behind every licensed childhood vaccine, it’s truly nauseating, as they report:
The below graph lists the vaccines recommended by CDC for routine use in children and shows the lack of a long-term placebo-controlled trial for each. Links to documentation are included which show the short safety review periods and the controls used.
Because of how limited safety testing is for vaccines prior to rolling them out to more than seventy million American children, the CDC relies on safety monitoring once vaccines are being given in the real world, which is where things get even more problematic.
Adverse Events Are Closer to One in Fifty
The 1986 law that indemnified vaccine makers from harm also created VAERS, which is a passive reporting system for vaccine adverse events. What this means is that VAERS only works to the extent doctors or parents decide to report a vaccine injury to the VAERS online system. Since most parents have no idea what a vaccine injury looks like and most doctors aren’t trained to recognize a vaccine injury, and the general stance is that vaccines are completely benign, you can imagine the limitations of this system, and science has born that out. In 2007 the CDC funded a study by Harvard Pilgrim Health Care for three years involving 715,000 patients that found “fewer than 1% of vaccine adverse events are reported.”
In 2016 VAERS received 59,117 reports of vaccine adverse events, including 432 deaths and 10,284 emergency room visits.
If those 59,117 reports were 1 percent of the actual total, that would imply there had actually been 5.9 million reportable adverse events from vaccines in a single year.
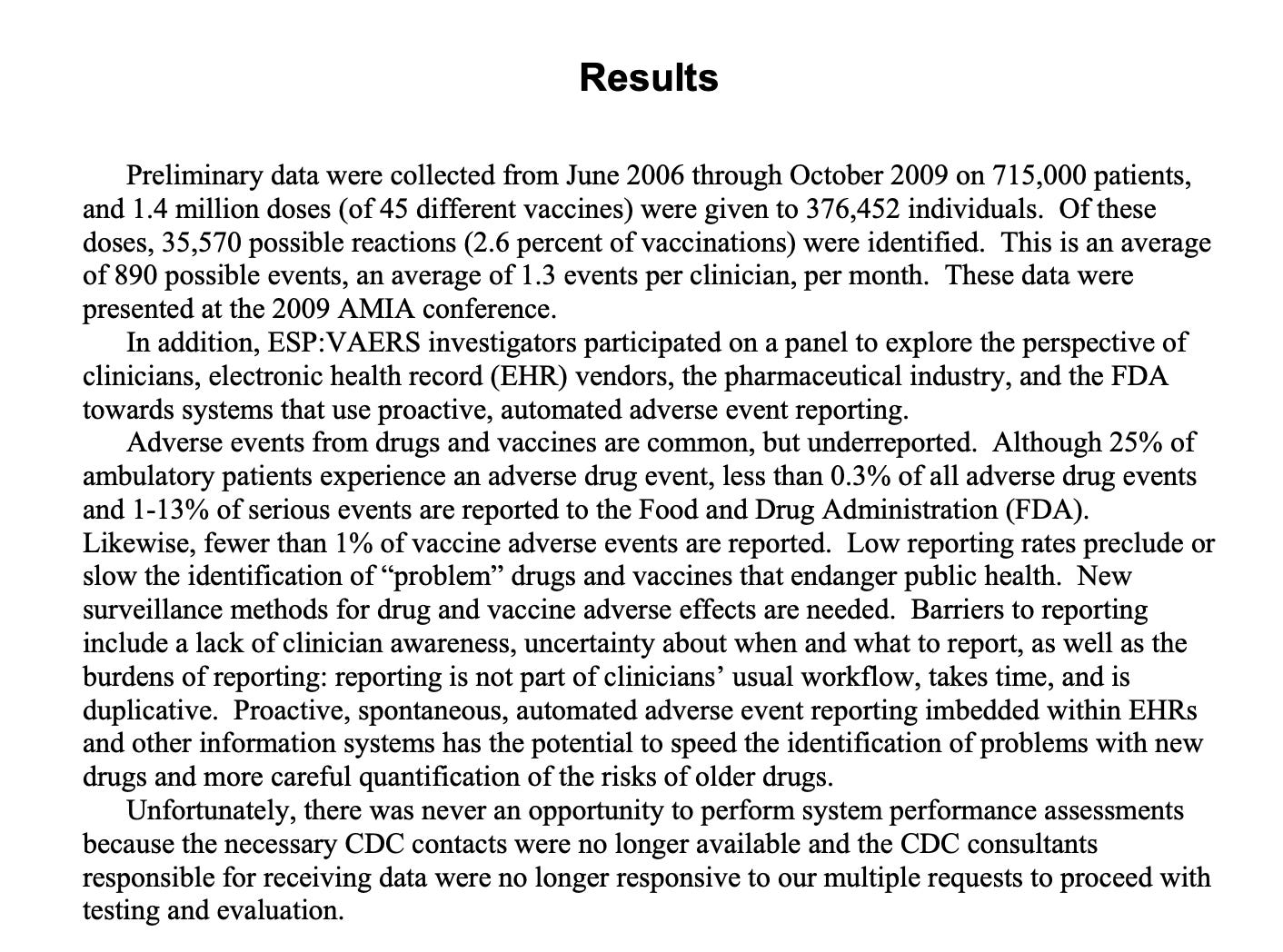
The CDC-funded Harvard Pilgrim study’s purpose was to automate the reporting of vaccine injuries by programming known vaccine reactions into medical charts of patients experiencing certain reactions near the time of vaccination. The pilot study yielded troubling results, because of 715,000 individuals, 35,570 possible vaccine reactions were identified. That’s 2.6 percent of vaccine recipients—a far cry from the “one in a million” figure tossed around by vaccine marketers! The Harvard Pilgrim researchers stood ready to integrate this new reporting system with VAERS but reported instead that the CDC went radio silent on a study that cost more than one million dollars, as principal investigator Ross Lazarus reported:
Unfortunately, there was never an opportunity to perform system performance assessments because the necessary CDC contacts were no longer available and the CDC consultants responsible for receiving data were no longer responsive to our multiple requests to proceed with testing and evaluation.
A three-year study produced results so potentially devastating to the CDC—because the adverse event rate was so much higher than anything the CDC could share with the public—that the program was shut down.
Adverse Events Are Poorly Understood
What harm, exactly, can a vaccine cause? In 1991 the prestigious Institute of Medicine (IOM) looked at side effects from just one vaccine, the DPT, and concluded that science supported a causal relationship with the following six vaccine injuries: acute encephalopathy, chronic arthritis, acute arthritis, shock and unusual shock-like state, anaphylaxis, and protracted inconsolable crying. In 2012 the IOM looked at the 158 most common vaccine injuries reported to VAERS and found that science “convincingly supports a causal relationship” with 18 of those injuries but found that there wasn’t any science to either confirm or deny 135 additional injuries. Here’s the list of injuries that might be caused by vaccines, except no one has looked:
Encephalitis, encephalopathy, infantile spasms, afebrile seizures, seizures, cerebellar ataxia, acute disseminated encephalomyelitis, transverse myelitis, optic neuritis, neuromyelitis optica, multiple sclerosis, Guillain-Barré syndrome, chronic inflammatory demyelinating polyneuropathy, brachial neuritis, amyotrophic lateral sclerosis, small fiber neuropathy, chronic urticaria, erythema nodosum, systemic lupus erythematosus, polyarteritis nodosa, psoriatic arthritis, reactive arthritis, rheumatoid arthritis, juvenile idiopathic arthritis, arthralgia, autoimmune hepatitis, stroke, chronic headache, fibromyalgia, sudden infant death syndrome, hearing loss, thrombocytopenia, immune thrombocytopenic purpura.
In 86 percent of the vaccine injuries reported to VAERS, no one has any idea whether they are related to vaccines.
No One Knows the True Impact of Multiple Doses
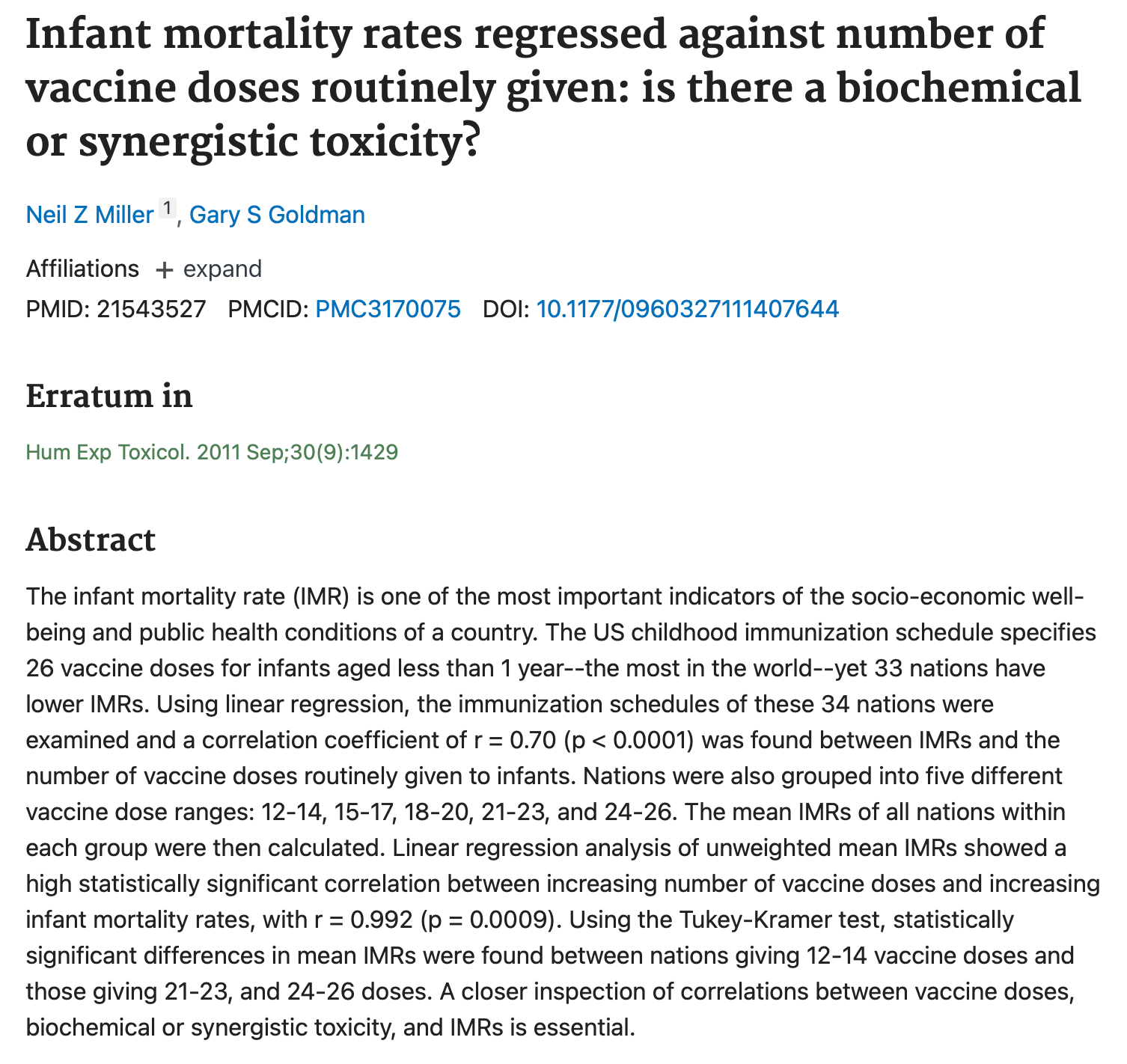
In 2012 a study looking at data from the aforementioned VAERS database noted several disturbing patterns. The more vaccines a child received in a single setting, the more likely she was to be hospitalized or die. In the study, published in Human and Experimental Toxicology, Dr. Gary Goldman and Neil Miller found a “a positive correlation between hospitalization rates and the number of vaccine doses” and also “younger infants were significantly more likely than older infants to be hospitalized or die after receiving vaccines.” The authors also affirmed the inadequacies of current vaccine testing:
Studies have not been conducted to determine the safety (or efficacy) of administering multiple vaccine doses in a variety of combinations as recommended by CDC guidelines.
Frustrating for parents is the contradictory, and scientifically unsupported, perspective the American Academy of Pediatrics provides on their website about vaccinating a child with multiple vaccines at once, which states: “Vaccines are well-studied to make sure that it is safe to give them all at once.” Parents are understandably confused.
The DTP Vaccine: More Harm than Good in Africa
There is little science comparing health outcomes of vaccinated children versus completely unvaccinated children; that is until 2017, when arguably the most disturbing science ever done on this topic produced an outcome that reflects very poorly on global vaccination efforts and asks and answers the ultimate question about vaccines: Are they really “safe and effective”? Published in the peer-reviewed journal EBioMedicine, the study is titled, “The Introduction of Diphtheria-Tetanus-Pertussis and Oral Polio Vaccine Among Young Infants in an Urban African Community: A Natural Experiment.”
Researchers from the Research Center for Vitamins and Vaccines, Statens Serum Institut (Denmark), and Bandim Health Project looked closely at data from the West African nation of Guinea-Bissau. The scientists in this study closely explored the concept of NSEs, “nonspecific effects” of vaccines, which is a fancy way of saying vaccines may make a child more susceptible to other infections. They found that the data for children who had been vaccinated with the DTP vaccine “was associated with 5-fold higher mortality than being unvaccinated. No prospective study has shown beneficial survival effects of DTP. . . . DTP is the most widely used vaccine. . . . All currently available evidence suggests that DTP vaccine may kill more children from other causes than it saves from diphtheria, tetanus, or pertussis. Though a vaccine protects children against the target disease, it may simultaneously increase susceptibility to unrelated infections.”
In lay terms, this means that giving a child the DTP vaccine may make the child sick from other infections. Life is about risk and reward. As a venture capital expert throughout my career, I used risk/reward to analyze every deal I ever made. Parents should have all the information they need, so that they too can make a risk/reward decision on behalf of their kids; in other words, informed consent. You and I and every other parent in the world want safety and health for our kids.
Perhaps no scientist has been more eloquent or public in discussing this issue than Dr. Tetyana Obukhanych, who wrote a book, Vaccine Illusion: How Vaccination Compromises Our Natural Immunity and What We Can Do to Regain Our Health, that discusses the issue of NSEs from vaccines. Dr. Obukhanych testified before the California State Assembly, just before they voted to make vaccines mandatory for school attendance in California. Her training is in immunology, and she herself would tell you that she began her education “very enthusiastic about the concept of vaccination, just like any typical immunologist.” However, Dr. Obukhanych quickly lost her enthusiasm for vaccinations, noting that
despite the fact that the biological basis of naturally acquired immunity is not understood, present day medical practices insist upon artificial manipulation of the immune response (a.k.a. immunization or vaccination) to secure “immunity” without going through the actual disease process. The vaccine-induced process, although not resembling a natural disease, is nevertheless still a disease process with its own risks. And it is not immunity that we gain via vaccination but a puny surrogate of immunity. For this reason, vaccination at its core is neither a safe nor an effective method of disease prevention.
What we learn from the African study, and that is perfectly explained by Dr. Obukhanych, is that children going through the artificial disease process triggered by a vaccine are actually more susceptible to suffer from (and sometimes die) from other diseases, because their immune system is weakened and compromised in ways we really don’t yet understand.
The Dengue Fever Vaccine
Another real-world example of the unanticipated NSEs from vaccines emerged from a scandal in the Philippines in late 2017. The dengue fever vaccine, administered to more than seven hundred thousand children, actually made dengue fever worse (and often deadly) for any vaccine recipients who hadn’t previously had dengue fever. The scandal engulfed the nation and prompted scathing condemnations of pharmaceutical industry influence by the president of the Philippines, Rodrigo Duterte, who stated through his spokesperson, “We will leave no stone unturned in making those responsible for this shameless public health scam which puts hundreds of thousands of young lives at risk accountable.” National Public Radio covered the scandal and reported:
The world’s only vaccine against dengue has hit a roadblock, and this complication is causing some countries to restrict use of the vaccine. Sanofi Pasteur, the French company that manufactures the shot, raised new safety concerns last week about the vaccine. In response, the Philippines suspended a mass immunization campaign, which has already given one dose of the vaccine to more than 700,000 children. And the Brazilian government has tightened restrictions on the shot. The vaccine—called Dengvaxia—raises the risk of a deadly form of dengue for people who have never been exposed to the virus, Sanofi Pasteur wrote Wednesday in a statement. The company says it discovered the complication after analyzing data from a six-year study. . . . Sanofi Pasteur has spent more than $1.5 billion to develop Dengvaxia over the past two decades. The vaccine is currently approved in 19 countries, including Costa Rica, El Salvador, Guatemala, Indonesia, Mexico and Thailand. The Philippines was leading the most ambitious — and costly — effort to vaccinate kids. More than 700,000 kids, older than age 9, had already received one dose. Over the next few years, the country had planned to give two more doses to the 700,000 kids who had already received one dose.
The Manila Times was highly critical of the dengue fever vaccine fiasco, blaming former Philippine president Aquino (who ordered the mass vaccination against dengue fever) and quoting dengue fever researcher Dr. Scott Halstead, who provided some dark irony: “It’s happened. We have a vaccine that enhances dengue.”
The Flu Vaccine Made Canadians More Vulnerable
It’s unlikely many Americans heard about the dengue fever vaccine scandal, and probably fewer still knew that a similar study in Canada had noted the phenomenon of a weakened immune response after being vaccinated back in 2015, this time involving the flu vaccine. University of Calgary researchers, profiled in an article in Global News titled, “Canadian study finds flu shot could increase risk of getting sick,” discovered that the 2014–15 flu vaccine worked far better for people who hadn’t received a flu vaccine in the previous year. Said differently, the more vaccines for flu you received, the less well it worked.
In the Global News article, University of Calgary researcher Dr. Jim Dickinson explained: “A negative effectiveness suggests the vaccine made people more susceptible to the flu. We need to do further research to understand why this has happened.”
Bolstering the case that repeated flu vaccines may alter the immune system in unpredictable ways, in 2018 University of Maryland scientists discovered that receiving a flu vaccine made your risk of infecting others far more likely, because the volume of flu vaccine you shed through breathing and sneezing was six times higher than for those who hadn’t received a flu vaccine:
[We found] 6.3 (95% CI 1.9–21.5) times more aerosol shedding among cases with vaccination in the current and previous season compared with having no vaccination in those two seasons.
Parents Are Concerned about Gardasil
Gardasil, a vaccine intended to prevent the spread of the human papilloma virus (HPV), is the most important new vaccine for Merck, the largest vaccine maker in the world. Gardasil alone accounted for more than two billion dollars in revenues in 2016, making Gardasil Merck’s single largest vaccine.
Gardasil is typically administered to healthy teenage girls, and the devastating stories of chronically ill and injured girls following Gardasil administration has crept up in every country where the vaccine is administered. In Japan, a country with a robust history of honesty about vaccine side effects, the stories of Gardasil injuries became such a public scandal that uptake rates for the vaccine are now under 1 percent (current rate in the United States is over 60 percent for teenage girls). In late 2016 a Japanese industry watchdog group—Medwatcher Japan—issued a scathing letter criticizing, among others, the World Health Organization, which they felt was endorsing the Gardasil vaccine without acknowledging the growing body of science demonstrating high rates of devastating side effects:
Countries other than Japan have also indicated major problems with the safety of HPV vaccines. Ignoring these “inconvenient” facts in an effort to promote HPV vaccination contradicts the primary responsibility of WHO, which is to dispassionately assess risks and benefits. . . . Reported serious AEs [adverse events] include diverse, complex, multi-system symptoms such as seizures; disturbance of consciousness; systemic pain including headache, myalgia, arthralgia, back pain and other pain; motor dysfunction such as paralysis, muscular weakness, exhaustion, and involuntary movements; numbness and sensory disturbance; autonomic symptoms including dizziness, hypotension, tachycardia, nausea, vomiting, and diarrhea; respiratory dysfunction including dyspnea and asthma; endocrine disorders such as menstrual disorder and hypermenorrhea; hypersensitivity to light and sound; psychological symptoms including anxiety, frustration, hallucinations, and overeating; higher brain dysfunction and cognitive impairments including memory impairment, disorientation, and loss of concentration; and sleep disorders, hypersomnia and sudden sleep attacks. In some cases, these symptoms impair learning and result in extreme fatigue and decreased motivation, negatively impacting everyday life.
Meanwhile, in Ireland the furious debate about Gardasil was frequently front page news throughout 2017 as a well-organized group of parents—calling themselves “Regret”—turned the debate about Gardasil into a national issue. In the late fall of 2017, the Irish Times reported that “uptake for the vaccine has plummeted from a high of 87 per cent to 50 per cent. Any further decline is likely to call into question the economic, medical and political rationale of the programme” and that “almost 650 girls in Ireland reported requiring medical intervention or treatment after receiving the HPV vaccine, according to data collected by the State’s medicines watchdog.”
In 2017 a published meta-analysis of Gardasil clinical trials stated that “two of the largest randomized trials found significantly more severe adverse events in the tested HPV vaccine arm of the study.” The study, “Serious adverse events after HPV vaccination: a critical review of randomized trials and post-marketing case series,” concluded, “These findings raise further doubt on HPV vaccine safety.”
Merck’s most important vaccine receiving withering, worldwide criticism may serve to accelerate a reckoning about vaccines in general and perhaps shed the light more fully on autism, too. Gardasil shares something in common with most of the vaccines given to infants: a very high level of aluminum adjuvant.
Vaccines Are Linked to Autoimmune Disease
Autism may just be the tip of the iceberg for a host of neurological and physical disorders impacting our children at epidemic levels. Conditions of autoimmunity—asthma, diabetes, food allergies, eczema, and so on—are growing at rates similar to autism. Could vaccines also be behind their explosion? According to many scientists, absolutely.
As one example, scientists at the University of Virginia have drawn a direct line between the aluminum (referred to as “alum”) used in vaccines to stimulate the immune system and the explosion in food allergies, stating “the era of food allergy began with the post-millennial generation, the same faction who received new immunizations during early childhood. Many of these vaccines contain alum, an adjuvant known to induce allergic phenotypes.” I wrote an extensive article about aluminum and autism right here:

Allergy scientists know that if they want to create a food allergy in rats, the quickest way to do it is by injecting them with vaccine ingredients. In a study from Norway—“Development and Characterization of an Effective Food Allergy Model in Brown Norway Rats”—scientists wanted to figure out the quickest way to give lab rats a food allergy so they could study various food allergy suppression drugs on them. Since rats aren’t born with food allergies, the most effective method was clear: inject the rats with egg protein and aluminum adjuvant, and they will soon be allergic to eggs.
There’s even a textbook from one of the largest textbook companies (Wiley & Sons) in the world titled Vaccines and Autoimmunity, a book that “explores the role of adjuvants—specifically aluminum in different vaccines—and how they can induce diverse autoimmune clinical manifestations in genetically prone individuals.” The book’s co-author, Dr. Yehuda Shoenfeld, is viewed as the world’s foremost authority on autoimmunity, and he is very direct in raising the alarm bell about vaccine side effects:
“Due to the adverse effects exerted by adjuvants, there is no controversy over the need for safer adjuvants for incorporation into future vaccines.”
Unvaccinated kids are…healthier, according to 6 studies
The first study that compared children who had received a vaccine with children that hadn’t was published in 2000. Although autism wasn’t something the study considered, it was still revealing. Titled “Effects of Diphtheria-Tetanus-Pertussis or Tetanus Vaccination on Allergies and Allergy-Related Respiratory Symptoms among Children and Adolescents in the United States,” this study from the UCLA school of public health did look specifically at the DTP vaccine to see if it might be responsible for allergies and allergy-related symptoms, such as asthma. Looking at more than thirteen thousand children, the study found that:
DTP or tetanus vaccination in US children is associated with lifetime history of asthma or other allergies and allergy-related symptoms. . . . Assuming that the estimated vaccination effect is unbiased, 50% of diagnosed asthma cases (2.93 million) in US children and adolescents would be prevented if the DTP or tetanus vaccination was not administered.
So the first study to ever compare a group that received a vaccine with a group that didn’t found a dramatic difference in rates of asthma and allergies among the vaccinated group, so much so that they thought not getting the DTP vaccine might reduce cases of asthma by 50 percent! Note that many children with autism suffer from what are known as comorbid conditions, such as asthma, allergies, and other autoimmune conditions.
In 2008 in the second study ever looking at a group of children who didn’t receive a vaccine, public health researchers Carolyn Gallagher and Melody Goodman from SUNY Stony Brook looked at the possible relationship between the hepatitis B vaccine and special education.Were children who received the full series of hepatitis B vaccines (three separate vaccines, the first one often given on day one of life) more likely to end up in special education classes than children who didn’t receive any hepatitis B vaccines? The study, “Hepatitis B Triple Series Vaccine and Developmental Disability in US Children Aged 1–9 Years,” was published in the journal Toxicological and Environmental Chemistry, and the results were pretty clear: The full series of hepatitis B led to a ninefold greater likelihood of receiving special education:
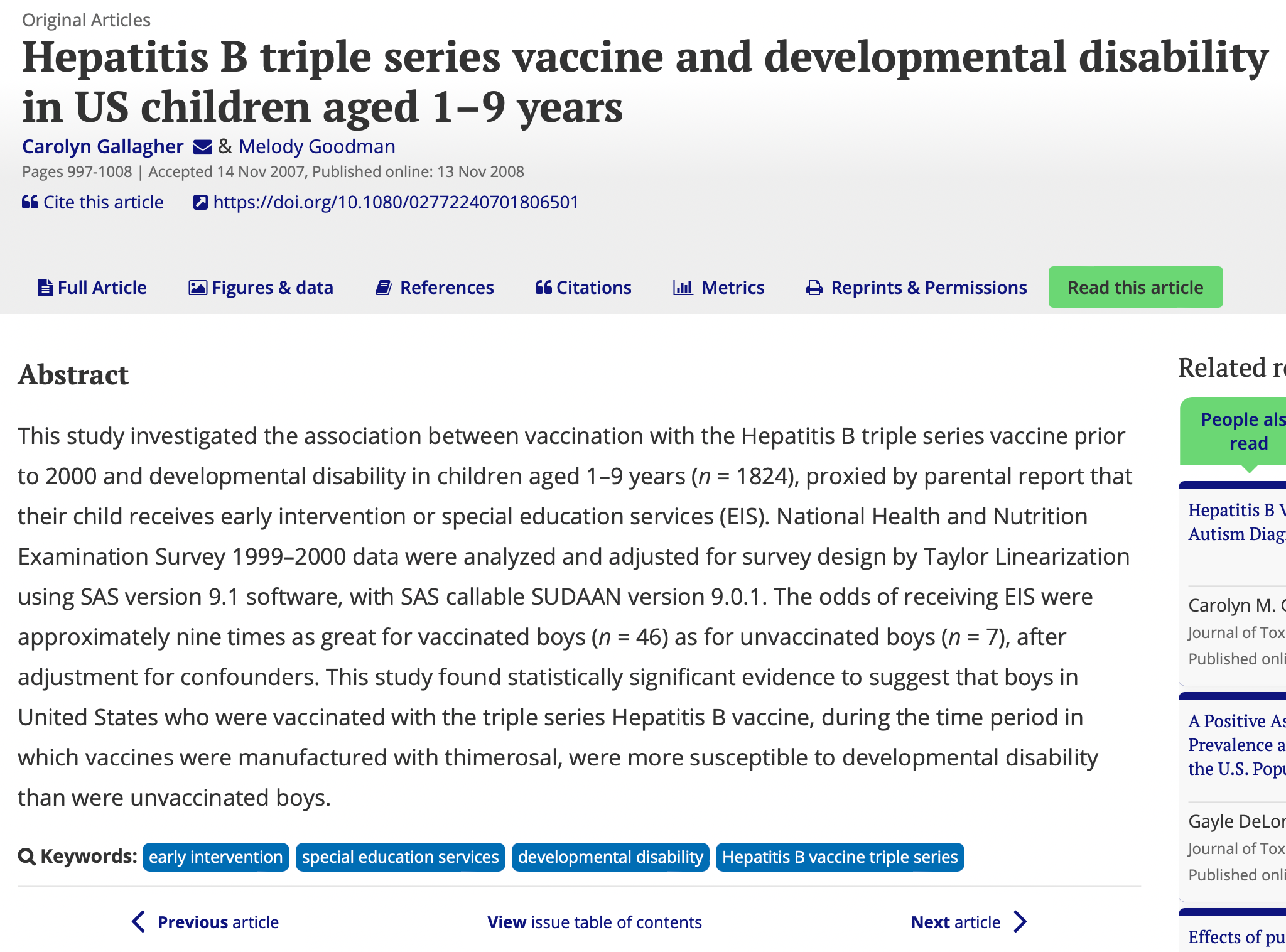
This study found statistically significant evidence to suggest that boys in United States who were vaccinated with the triple series Hepatitis B vaccine . . . were more susceptible to developmental disability than were unvaccinated boys. . . . The odds of receiving EIS [special education] were approximately nine times as great for vaccinated boys (n = 46) as for unvaccinated boys (n = 7), after adjustment for confounders.
The same researchers from SUNY Stony Brook published another study in 2010, this time looking at the relationship between receiving the hepatitis B series and autism. Published in the prestigious Journal of Toxicology and Environmental Health, “Hepatitis B Vaccination of Male Neonates and Autism Diagnosis” once again reached very clear conclusions:
“Boys vaccinated as neonates had threefold greater odds for autism diagnosis compared to boys never vaccinated or vaccinated after the first month of life.”
Journalist David Kirby appreciated the significance of the new findings, writing in the Huffington Post:
[The study] will be among the first university-based population studies to suggest an association between a vaccine and an increased risk for autism. And that would be in direct contradiction to all those MMR and thimerosal studies that purportedly found no such link.
The two Goodman and Gallagher articles about hepatitis B raise many concerns. I’ve met pediatricians who feel that the hepatitis B vaccine specifically has triggered the epidemic of neurological disorders and autoimmunity we now see in our children. Hepatitis B was the first vaccine introduced after Congress indemnified vaccine makers from liability in 1986. The vaccine has a high dose of aluminum, which I believe is the primary cause of autism and it’s often given to babies on day one of life, which many immunologists feel is a huge mistake. These two studies raise major concerns, but I’m guessing you never knew either of these studies existed, which supports my point about scientists and PR firms.
In 2017, however, something amazing happened. Two separate studies comparing vaccinated and completely unvaccinated children actually got published. Unlike the Goodman and Gallagher studies above, which only explored a single vaccine (the rest of a child’s vaccine status was simply not considered), these two new studies met the “gold standard”—they found children who had never received any vaccines and looked at their health outcomes in a variety of ways. The public health researchers from Jackson State University originally planned to publish a single study, until they looked at the data on children born prematurely, noting that the data on the difference in health outcomes for vaccinated versus unvaccinated premature infants was so dramatic it deserved its own study.
Published in the Journal of Translational Science, the first groundbreaking study was called, “Pilot Comparative Study on the Health of Vaccinated and Unvaccinated 6- to 12-Year-Old U.S. Children,” and its results were so devastating to the US vaccine program that there wasn’t a single media outlet in the country that covered its release. The results of comparing vaccinated children to completely unvaccinated children were no surprise to me, my wife, or any of the autism parents I know, but perhaps would surprise others:

The vaccinated were less likely than the unvaccinated to have been diagnosed with chickenpox and pertussis, but more likely to have been diagnosed with pneumonia, otitis media, allergies and NDD [neurodevelopmental disorders]. After adjustment, vaccination, male gender, and preterm birth remained significantly associated with NDD.
Specifically, vaccinated children were found to have a fourfold higher likelihood of having autism. I’m reminded of a quote by Dr. Daniel Neides of the Cleveland Clinic, who wondered if we were making trade-offs that aren’t worth it. He said,
“Some of the vaccines have helped reduce the incidence of childhood communicable diseases [like chickenpox and pertussis from the study above] . . . but not at the expense of neurologic diseases like autism and ADHD increasing at alarming rates.”
Simultaneously, the Jackson State authors published a study in the same journal just looking at children born prematurely, titled, “Preterm Birth, Vaccination and Neurodevelopmental Disorders: A Cross-Sectional Study of 6- to 12-Year-Old Vaccinated and Unvaccinated Children.” The results were disturbing, as the researchers found children born prematurely and vaccinated were fourteen times more likely to develop a neurodevelopmental disorder! The authors were appropriately concerned:
Preterm birth coupled with vaccination, however, was associated with a synergistic increase in the odds of NDD, suggesting the possibility that vaccination could precipitate adverse neurodevelopmental outcomes in preterm infants. These results provide clues to the epidemiology and causation of NDD but question the safety of current vaccination programs for preterm infants.
In 2020, Dr Brian Hooker Neil Miller took the study of unvaccinated children to a new level by looking at actual data from a pediatrician’s office who had a large number of unvaccinated patients. The study, Analysis of health outcomes in vaccinated and unvaccinated children: Developmental delays, asthma, ear infections and gastrointestinal disordersconcluded exactly what by now is a pretty familiar refrain:
Vaccination before 1 year of age was associated with increased odds of developmental delays (OR = 2.18, 95% CI 1.47-3.24), asthma (OR = 4.49, 95% CI 2.04-9.88) and ear infections (OR = 2.13, 95% CI 1.63-2.78). In a quartile analysis, subjects were grouped by number of vaccine doses received in the first year of life. Higher odds ratios were observed in Quartiles 3 and 4 (where more vaccine doses were received) for all four health conditions considered, as compared to Quartile 1. In a temporal analysis, developmental delays showed a linear increase as the age cut-offs increased from 6 to 12 to 18 to 24 months of age (ORs = 1.95, 2.18, 2.92 and 3.51, respectively). Slightly higher ORs were also observed for all four health conditions when time permitted for a diagnosis was extended from ⩾ 3 years of age to ⩾ 5 years of age.
Conclusion: In this study, which only allowed for the calculation of unadjusted observational associations, higher ORs were observed within the vaccinated versus unvaccinated group for developmental delays, asthma and ear infections. Further study is necessary to understand the full spectrum of health effects associated with childhood vaccination.
Six separate studies, all comparing a group of children vaccinated with a group of children unvaccinated, at least for a single vaccine. I’m guessing that for most readers this is the first time you’ve read about any of these studies. I think a fair question would be, “Why?” The answer is simple: Studies that might hurt the financial performance of pharmaceutical companies or damage the reputation of public health officials or embarrass pediatricians are not publicized by media outlets that derive advertising revenue from the pharmaceutical companies.
Vaccines Didn’t Cause the Decline in Measles
The idea that vaccines saved humanity is unsupportable by the facts. But it’s worth addressing the two diseases that everyone talks about whenever a vaccine debate takes place: measles and polio. I’ll start with measles.
Just before the first rollout of a nationwide measles vaccine program, the three leading scientists at what was then called the Public Health Service (today’s CDC) made a presentation in San Francisco at the American Public Health Association’s annual meeting. The date was November 1, 1966. The presentation was led by Dr. David J. Sencer, who at the time held the title of chief of the PHS’s National Communicable Disease Center. He was joined by his assistant chief, Dr. H. Bruce Dull, as well as the PHS’s chief of epidemiology, Dr. Alexander Langmuir. It’s fair to say that at this point in history no one knew more about the measles virus than these three scientists. The PHS scientists used the APHA’s annual meeting to announce plans for their ambitious national launch, with the hopes of eradicating measles by the end of 1967.
The doctors also turned their presentation into a report titled, “Epidemiological Basis for Eradication of Measles in 1967,” and some of the matter-of-fact statements they made might get a doctor banned from the mainstream media today as even a single case of measles is a cause for panic and outbreak stories often make the national news. In fact, a new parent might think measles was just like Ebola, except it’s not, as the PHS scientists made very clear in 1966 stating,
“For centuries the measles virus has maintained a remarkably stable ecological relationship with man. The clinical disease is a characteristic syndrome of notable constancy and only moderate severity. Complications are infrequent, and, with adequate medical care, fatality is rare.”
In the 1950s and ’60s, even without vaccines, measles outbreaks only happened every few years, on a somewhat dependable cycle; they noted that “in large population centers, as in cities or whole metropolitan areas, measles epidemics recur in 2-to-3-year cycles.” They also established a vaccination threshold to eradicate measles well below the 95 percent number public health officials use today, nothing that “it is evident that when the level of immunity was higher than 55 percent, epidemics did not develop.” Before the vaccine had been introduced, it’s worth noting that the death rate from measles in the United States had already declined by approximately 99.96 percent from its peak in the mid-1800s. In 1960 the death rate from measles was 0.23 per 100,000 people. Asthma, by comparison, had a mortality rate more than ten times higher for the same year.
In 2013 “Measles Vaccination Before the Measles-Mumps-Rubella Vaccine” was published in the American Journal of Public Health, looking at the history of the measles vaccine, and had many similar observations about the history of measles, including the view from parents and doctors that measles was “unpleasant but inevitable”:
At the beginning of the 1960s, it was clear that a vaccine against measles would soon be available. Although measles was (and remains) a killer disease in the developing world, in the United States and Western Europe this was no longer so. Many parents and many medical practitioners considered measles an inevitable stage of a child’s development. . . . By 1960, thanks to the use of antibiotics and improvements in living conditions, measles mortality was declining steadily in industrialized countries. . . . Parents largely came to see measles as an unpleasant, although more or less inevitable, part of childhood. Many primary care physicians shared this view.
“So what?” some might argue, even if measles was considered a mild and inevitable illness of childhood, aren’t we better off as a society by having even less measles around? But I think we should all be suspicious of the extreme fear-mongering generated in the press every time even a single case of measles surfaces and ask the question, “Who is generating all the panic?” Also, we have to be honest about the adverse events from the MMR vaccine and decide if they outweigh the benefits of reducing the incidence of a mild childhood illness. According to Physicians for Informed Consent, a large group of doctors in California:
There is no evidence that the measles vaccine causes less death or permanent disability than measles. The vaccine package insert raises questions about safety testing for cancer, genetic mutations, and impaired fertility. Although VAERS tracks some adverse events, it is too inaccurate to measure against the risk of measles. Clinical trials do not have the ability to detect less common adverse reactions, and epidemiological studies are limited by the effects of chance and possible confounders. Safety studies of the measles vaccine are particularly lacking in statistical power. A review of more than 60 measles vaccine studies conducted for the Cochrane Library states, “The design and reporting of safety outcomes in MMR vaccine studies, both pre- and post-marketing, are largely inadequate.” Because permanent sequalae (after effects) from measles, especially in individuals with normal levels of vitamin A, are so rare, the level of accuracy of the research studies available is insufficient to prove that the vaccine causes less death or permanent injury than measles.
That’s quite a statement from a group of doctors. They’re saying the risk/reward equation to have the measles vaccine isn’t there.
What about Polio?
It wouldn’t be an exaggeration to say that the modern vaccine industry was built on the reputation the polio vaccine carries forth to this day for having saved the children of the world from the scourge of polio. Nothing stirs the emotions quite like polio, especially for anyone who lived through the polio scares of the 1940s and ’50s. The images of children in iron lungs, casts, and using crutches to walk is the most chilling imagery we have of any infectious disease in the modern era, and polio is always referenced whenever debates about vaccines erupt.
Ending the polio epidemic is the iconic achievement of vaccines, and maintaining the purity and simplicity of the narrative that vaccines ended the polio epidemic is critical to maintaining the image of vaccines as infallible and essential. That being said, there are several unanswered questions about polio that deeply challenge the narrative that the polio vaccine saved the world:
Why did poliovirus, a well-known and fairly mild enterovirus, suddenly provoke a devastating epidemic in the late 1940s and early 1950s? For most, a bout with poliovirus is a minor event, but for a small number (perhaps 1 to 2 percent), the virus somehow makes its way into the nervous system, where it can be far more dangerous, and sometimes deadly poliomyelitis. The outbreaks were confined largely to warm-weather months. They had higher prevalence in agricultural areas. Do any of these facts relate to each other?
Did DDT escort poliovirus into the nervous system? In November 1953 Dr. Morton S. Biskind published a pretty clear answer in the American Journal of Digestive Diseases.His famous paper, “Public Health Aspects of the New Insecticides,” minced absolutely no words in making it clear what was causing mild poliovirus to morph into paralytic poliomyelitis: DDT. The insecticide, utilized for the first time in 1945, had become ubiquitous in the United States, even though the public health service warned in 1951 how risky its use was: “
DDT is a delayed-action poison. Due to the fact that it accumulates in the body tissues, especially in females, the repeated inhalation or ingestion of DDT constitutes a distinct health hazard. The deleterious effects are manifested principally in the liver, spleen, kidneys, and spinal cord. . . . Children and infants especially are much more susceptible to poisoning than adults.”
Can DDT use explain the trends in polio outbreaks? DDT spraying was much more prevalent in the warm-weather months. Many of the first cases of polio took place in agricultural areas. There were many case examples to compare and contrast: Israel, which was late in introducing DDT (in the early 1950s), was late in having a polio epidemic.I n the Philippines, American troops used DDT on the military bases and had high poliomyelitis outbreaks, but natives living outside the base didn’t.
Most importantly, Dr. Biskind explained in his article that the biological science published in 1944 and 1947 showed that DDT did the very thing that made the nervous system susceptible to poliovirus’s becoming poliomyelitis: It produced “degeneration of the anterior horn cells of the spinal cord in animals.” These cells at the top of the spinal column are the key entry point to the spinal column, where the poliovirus then creates inflammation of the myelin sheath creating, you got it, poliomyelitis.
Once biological plausibility was firmly established, Dr. Biskind then asked in his article the most important question about the polio epidemic you’ve never heard before: “When the population is exposed to a chemical agent known to produce in animals lesions in the spinal cord resembling those in human polio, and thereafter the latter disease increases sharply in incidence and maintains its epidemic character year after year, is it unreasonable to suspect an etiologic relationship?”
Why does polio stubbornly persist in countries like India, even though many Indian children are vaccinated fifteen or more times before the age of five? Perhaps it also won’t surprise you that in India, where polio stubbornly persists even with children receiving as many as two dozen polio vaccines each, DDT remains in wide use.
Did polio decline in near lockstep with the decline and ultimate ban of DDT in the United States? Yes, it did. The United States, in fact, hasn’t had a case of polio since 1979. DDT was banned by the EPA in 1972.
Could “polio provocation” also explain the rise in polio? What’s clear about poliovirus’s becoming poliomyelitis is that somehow the virus needs to be able to jump into the nervous system. DDT appears to be a potent escort, given its capacity to degenerate the spinal cord. Another potential escort is what’s known as “polio provocation,” a theory that recently moved from hypothesis to biological fact. An article from Cambridge University explains: “In 1998 scientists Drs Matthias Gromeier and Eckard Wimmer were able to show that tissue injury caused by certain injections gives the polio virus easy access to nerve channels, thereby increasing its ability to cause paralysis.”
The study, “Mechanism of Injury-Provoked Poliomyelitis,”explained: “Using a mouse model developed for the study of poliomyelitis, we have shown that muscular trauma induced by multiple injections can lead to rapid progression of PV-induced paralysis, upregulation of viral replication in certain tissues, and acceleration of the progression of histopathological lesions. Thus, our data provide direct experimental evidence for the concept of PPM [provocation poliomyelitis].”
The study authors raised a very concerning question: What if the very act of repeated vaccination was the thing leading to poliomyelitis in the developing world?
“Skeletal muscle injury is known to predispose its sufferers to neurological complications of concurrent poliovirus infections. This phenomenon, labeled ‘provocation poliomyelitis,’ continues to cause numerous cases of childhood paralysis due to the administration of unnecessary injections to children in areas where poliovirus is endemic. Recently, it has been reported that intramuscular injections may also increase the likelihood of vaccine-associated paralytic poliomyelitis in recipients of live attenuated poliovirus vaccines.”
During the 1950s, tonsillectomy surgeries on children also exploded, and children who had received the operation were three times likelier to develop polio.
The elimination of DDT may have had as much, if not more, to do with the reduction of polio cases in the United States as the vaccine did. A blog post titled “The Age of Polio” by journalist Dan Olmsted and autism father Mark Blaxill considered this very issue, wondering if the narrative we’ve been fed about polio is too simplistic, the authors arguing “that a single-minded focus on germs—and an unwillingness to explore novel and potentially uncomfortable ideas from outside medical orthodoxy [such as DDT’s being a trigger for poliomyelitis]—is an inadequate strategy when it comes to modern diseases.” Worse, the simplistic view that epidemics such as polio’s can be conquered solely with a vaccine might inhibit a more holistic understanding of how to fight disease:
But the victory over the epidemics of poliomyelitis means our understanding of polio is essentially frozen in amber, circa 1955. Few diseases have been so completely conquered, at least at home, while being so incompletely understood, and that is not a good outcome. In leaving so many important topics on the table — why outbreaks occurred, why the pattern of contagion was so atypical for an infectious disease — scientists allowed some weak ideas to become conventional wisdom and some important ones to be missed. . . . And the connection of other illnesses to pesticides, and environmental toxins in general, has been slow in dawning. . . . The suffering of polio’s victims is honored by learning all of its lessons, including the danger of environmental toxins and the perils of ignoring their role in modern disease; the risk of focusing all of our energy on vaccinations as magic bullets, and the fundamental ethical obligation to search for the truth without fear or favor. Only then can we work out the real nature of illnesses that confront us here and now, ranging from autism to Parkinson’s to the persistence of poliomyelitis itself. Only then can we begin to prevent such disasters as The Age of Polio.
I’m sure some are wondering, If I can even criticize the polio vaccine, am I really just saying that no vaccines are worth it? I think each vaccine needs to be evaluated on its own merits. Much as Physicians for Informed Consent did with their analysis of the data, sometimes the risks from a vaccine outweigh the potential benefits, but these facts are very hard for the average parent to ascertain. And the history of vaccination needs to be accounted for in a more honest and transparent manner. Finally, the relationship between man and infectious disease is likely far more complicated and intertwined than we all appreciate.
What if there was a synergistic component to having certain illnesses, meaning they actually made your immune system more robust in the long term? That may sound esoteric to you, but scientists are aggressively pursuing just this angle, and the results are thought-provoking. A 2010 study, “Mumps and Ovarian Cancer: Modern Interpretation of an Historic Association,” found that having had mumps (the other “M” of the MMR vaccine) might make someone less susceptible to ovarian cancer. A 1998 study found that children who had measles and other “febrile infectious childhood diseases” had lower cancer risk as adults. A 2000 British Journal of Cancer study found that measles in childhood led to a lower risk of Hodgkin’s disease and that having childhood illnesses in general created lower cancer rates: “these results support previous evidence that early exposure to infection protects against HD [Hodgkin’s Disease].” A 2005 study by scientists from Canada examined many studies and found, “infections may play a paradoxical role in cancer development with chronic infections often being tumorigenic and acute infections being antagonistic to cancer,” meaning exposure to infectious childhood diseases lowers cancer risk. And in 2016 Baylor scientists “reported an inverse relationship between a history of chicken pox and glioma, a type of brain cancer, meaning that children who have had the chicken pox may be less likely to develop brain cancer.”What if certain illnesses and our immune system really do have a synergistic relationship? What if nature is actually more complicated than we think?
There may be many parents who feel, even after understanding the true history of polio, compelled to get the polio vaccine for their child. I have no personal problem with that. My problem is with the exaggerated, one-sided, fault-free history of vaccines that parents are presented with, one that hits parents over the head with the “safe and effective” mantra and discourages critical thinking. And if we can’t talk honestly about vaccines, we really can’t talk about how to end the autism epidemic. And that’s my real beef. It has turned me into an angry father.
A Perfect Circle of Denial
Vaccine injury, in my opinion, hides in plain sight, largely due to the way vaccines are tested and monitored, which is compounded by how poorly understood vaccine injuries are by the typical first line of defense when problems happen: pediatricians. Let’s think through this perfect “circle of denial” for a moment:
Vaccines are tested, as single doses, by observing side effects for just a few days after they are given. This ensures that any conditions that take time to manifest, which would be most autoimmune and neurological conditions, will never be captured through safety testing. Next, the postadministration form of capturing adverse events, VAERS, has been shown to capture less than 1 percent of all vaccine injuries. Add to this that pediatricians are never taught how to identify vaccine injuries, partially because the safety testing and reporting are so inadequate. And finally, parents are left completely in the dark about what’s happening when their child has a reaction. When you think about this circle of denial, you can see how an epidemic of vaccine injuries could be hiding in plain sight.
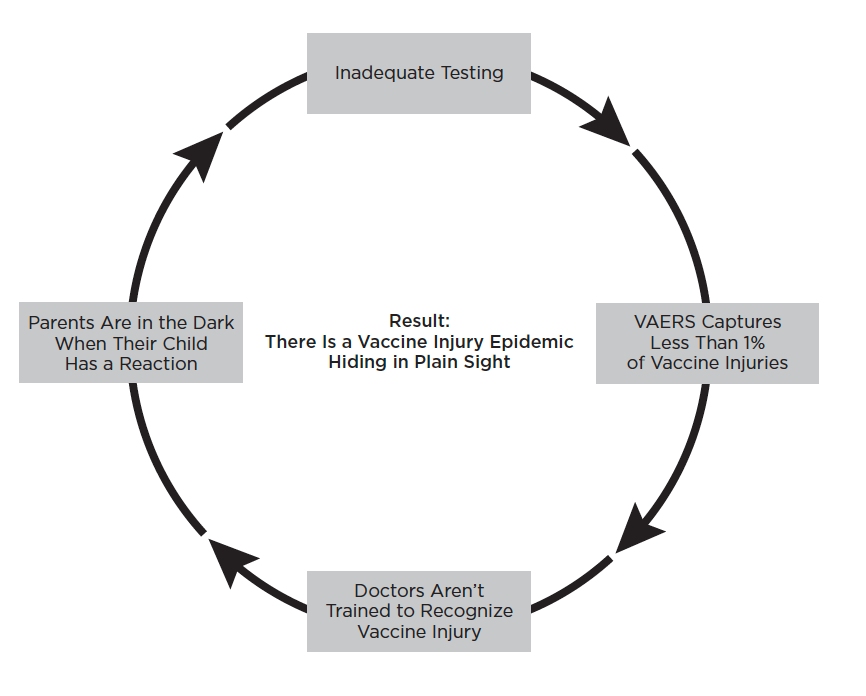
Doctors Are Raising Concerns
When I started to closely research vaccines after I watched my son’s health decline, I was shocked by how many doctors and scientists had raised very public concerns about whether vaccines are really “safe and effective” and had been doing so for decades. Dr. Robert Mendelsohn was the most famous American pediatrician of the 1970s and ’80s. He made over five hundred TV and radio appearances, authored six best-selling books about medicine and pediatrics that sold over a million copies, and wrote a nationally syndicated column, The People’s Doctor, for twelve years. Over those years his writing on the topic increased accordingly, and he told his readers that “although I administered them myself during my early years of practice, I have become a steadfast opponent of mass inoculations because of the myriad hazards they present.” He also realized that railing against the false narratives the vaccine industry had helped create would be hard for many to understand:
As I write about the dangers of mass immunization, that it is a concept that you may find difficult to accept. Immunizations have been so artfully and aggressively marketed that most parents believe them to be the “miracle” that has eliminated many once-feared diseases. Consequently, for anyone to oppose them borders on the foolhardy. For a pediatrician to attack what has become the “bread and butter” of pediatric practice is equivalent to a priest’s denying the infallibility of the pope.
Dr. Mendelsohn passed away in 1988, just as the United States was embarking on a massive campaign to increase the total number of vaccines given to children. He was the first nationally known pediatrician to express public concern about the growing hazards vaccines were creating, but he was far from the last. Perhaps the most well-known pediatrician today is California’s Dr. Robert Sears, whose 2008 book, The Vaccine Book: Making the Right Decision for Your Child, has sold more than 250,000 copies, and he provides some perspective on why he speaks out about the risks of vaccines:
I got interested in the topic of vaccines way back in medical school. A friend of mine convinced me to read a book about vaccines, and it ended up being a very anti-vaccine book. It was all about an old vaccine called the DPT vaccine that we don’t use anymore. But the book talked a lot about the risks and the dangers of that vaccine. The author of that book was calling for that vaccine to no longer be used. A number of years later, it turns out that they did discover that vaccine was causing a lot of very severe, life-threatening, even fatal side effects, so they did end up taking that vaccine off the market. So it kind of opened my eyes to the fact that there are some very severe, fortunately very rare, side effects to vaccines, and I wanted to learn more about this issue. I started reading a lot more books.[
Dr. Sears is joined by many other pediatricians, including pediatrician Dr. Lawrence Palevsky of New York, who provides some insight into what he learned about vaccines during medical school:
When I went through medical school, I was taught that vaccines were completely safe and completely effective, and I had no reason to believe otherwise. All the information that I was taught was pretty standard in all the medical schools and the teachings and scientific literature throughout the country. . . . Over the years, I kept practicing medicine and using vaccines and thinking that my approach to vaccines was completely onboard with everything else I was taught. But more and more, I kept seeing that my experience of the world, my experience in using and reading about vaccines, and hearing what parents were saying about vaccines were very different from what I was taught in medical school and my residency training . . . and it became clearer to me as I read the research, listened to more and more parents, and found other practitioners who also shared the same concern that vaccines had not been completely proven safe or even completely effective, based on the literature that we have today. . . . It didn’t appear that the scientific studies that we were given were actually appropriately designed to prove and test the safety and efficacy.
Dr. Suzanne Humphries, a board-certified nephrologist turned activist and the author of Dissolving Illusions, shared some perspective on her journey:
Do you know how much doctors learn about vaccines in medical school? When we participate in pediatrics training, we learn that vaccines need to be given on schedule. We learn that smallpox and polio were eliminated by vaccines. We learn that there’s no need to know how to treat diphtheria, because we won’t see it again anyway. We are indoctrinated with the mantra that “vaccines are safe and effective”—neither of which is true. Doctors today are given extensive training on how to talk to “hesitant” parents—how to frighten them by vastly inflating the risks during natural infection. They are trained on the necessity of twisting parents’ arms to conform, or fire them from their practices. Doctors are trained that nothing bad should be said about any vaccine, period.
Dr. Rachael Ross spent three seasons cohosting the Emmy Award–winning and nationally syndicated TV Show, The Doctors. When she wasn’t hosting the show, Dr. Ross was commuting home to run her family practice in Gary, Indiana, alongside her father and brother, both physicians. When Dr. Ross changed her tune about using vaccines in her practice, the mainstream media met her announcement with silence, but her words were powerful and clear. In 2016 Dr. Ross explained her change of heart in a widely read blog post titled, “Vaccines, Vaccine Injury, & My Perspective as a Doctor & Mom”.
I have witnessed the vaccine schedule grow from 16 doses of 4 vaccines from birth to six years old when I was a child, to the current recommendation of 49 doses of 14 vaccines between birth and age six, and 69 doses of 16 vaccines between birth and the age of eighteen . . . and we’ve been giving them on-time, sometimes five shots a day to help kids “catch-up,” and all without question. Medical school and residency taught us all to do so. I guess I can’t help but wonder if there’s a connection between the fact that when we had to give fewer vaccines we had fewer childhood diseases. It is only human to wonder. We had fewer learning disabilities, less asthma, less autism, and less diabetes. Autism in particular was 1 in 500 in the late seventies and it has now skyrocketed to 1 in 50. Why so many? Why so soon?
Dr. Ross’s concern, when you look at a chart of the data, is deeply disturbing; the linear relationship between the rise in vaccines and the rise in autism is hard to miss
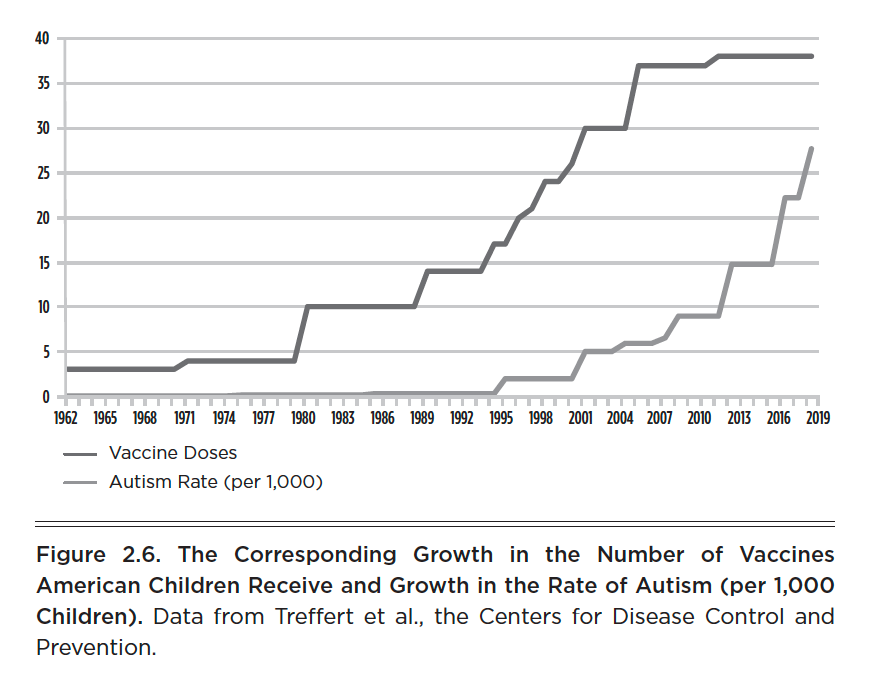
In early 2017 Dr. Daniel Neides, the medical director of Cleveland Clinic Wellness Institute caused a controversy when he wrote an article for the Cleveland Plain Dealer titled, “Make 2017 the year to avoid toxins (good luck) and master your domain: Words on Wellness.” He specifically addressed whether the risk/reward of the current vaccination program was worth it: “Some of the vaccines have helped reduce the incidence of childhood communicable diseases . . . but not at the expense of neurologic diseases like autism and ADHD increasing at alarming rates.”
I agree with Dr. Neides. In many cases I don’t think the vaccine trade-off is worth it. I think we’re swapping a minor reduction in a handful of acute illnesses for an explosion in lifelong chronic illness, including some as devastating as autism. But worst of all, I deeply resent the people in positions of authority and power who endlessly repeat the lie that vaccines are “safe and effective,” which serves to not only shame parents, but also to shut down an open debate. If we can’t honestly look at the facts about vaccines and recognize that they have real risks as well as some benefits, we will never be able to openly and honestly discuss the autism epidemic.
So, what are parents supposed to do?
Well, at the very least, I think the current CDC childhood schedule should not be followed. I think we should immediately reduce the total number of vaccines given to American children. The word “vaccinate” can mean so many different things, and not all vaccines are created equally. So it’s time to get specific, and it’s time to reduce the number of vaccines American children receive. First, if other first-world countries haven’t added a vaccine to their schedule, why should we give it to American children? Second, any vaccine added since the 1986 law removing liability from vaccine manufacturers is up for discussion. And third, if science exists implicating a vaccine or showing it’s done more harm than good, that’s a serious red flag.
In the United States there are thirteen separate vaccines currently on the US schedule, most given to children between two and four times each. They are: (1) hepatitis B, (2) rotavirus, (3) DTaP, (4) Hib, (5) PCV, (6) polio, (7) influenza, (8) MMR, (9) varicella, (10) hepatitis A, (11) meningococcal, (12) Tdap, (13) HPV.
Many first-world countries don’t give: hepatitis B (unless the mother is hepatitis B positive), rotavirus, influenza, varicella, hepatitis A, and HPV. So that simple exercise would remove six vaccines from the US schedule.
New since 1986 (and not already excluded): Hib, PCV, meningococcal. Hib is a potentially deadly bacteria. It’s particularly dangerous for infants. That said, the Hib vaccine contains aluminum, so the risk/benefit equation is complex. PCV (often called “prevnar”) has too many questions associated with it, including the possibility that PCV vaccines are contributing to antibiotic resistance and the explosion in methicillin-resistant Staphylococcus aureus (MRSA) cases. It should be removed. Meningococcal is a very new vaccine, only added to the schedule in 2012 for young children. Serious questions remain about its safety and efficacy. I would remove it.
Conclusion: Reduce the vaccine schedule to the following vaccines: DTaP, Hib, polio, and MMR. Of course, this will be viewed by pro-vaccine talking heads as a radical and dangerous idea, despite the fact that until the late 1980s, the entire US vaccine schedule was DTaP, polio, and MMR. Furthermore, decisions need to be made about when, exactly, to give these vaccines. In general, first vaccines should be delayed until children have reached their first birthday and the MMR delayed until they are past three years old, as Dr. Paul Thomas does in his practice. Speaking of Dr. Thomas, I really hope you listen to podcast I did with him where we discuss many of these issues:

I emailed this story to a friend, probably the only person in the world I think knows more about vaccines than I do. I asked him what he thought I should tell parents to do. He gave me a one word answer: “None.”
When it comes to vaccines, parents have much to ponder.
About the author

J.B. Handley is the proud father of a child with Autism. He spent his career in the private equity industry and received his undergraduate degree with honors from Stanford University. His first book, How to End the Autism Epidemic, was published in September 2018. The book has sold more than 75,000 copies, was an NPD Bookscan and Publisher’s Weekly Bestseller, broke the Top 40 on Amazon, and has more than 1,000 Five-star reviews. Mr. Handley and his nonspeaking son are also the authors of Underestimated: An Autism Miracle and co-produced the film SPELLERS, available now on YouTube.
The most basic understanding of physiology combined with a basic understanding of how vaccines are made, what they contain and what they are designed to do, should raise questions in any parent. Vaccination took off in an age when faith in the medical industry and science was great. Older generations had a basic understanding of health, disease and the human organism and immune function. Younger generations transferred all faith to science-medicine because of decades of propaganda promoting the idea that only in the hands of a doctor could you and your child be safe.
And as you say, in the beginning there were not many vaccinations and there was very little pressure. I had children in the early Seventies in Australia and the only vaccine they had was for Polio. In my early Twenties I had not done the research I should have done and if I had done it, would never have allowed that one vaccination.
We lived in a country town and the young doctor, in his late Twenties, still gave the same advice my parents had received - expose your kids to Measles, Mumps, Chicken Pox and let them get it, get over it and have lifelong immunity. So I did. My children were fine as I, my siblings, friends, schoolmates had all been fine in the 1950's. Following more than half a century of brainwashing, I doubt young parents today, or even old ones, could comprehend that health lies not in a needle or a pill, or in artificially reducing every temperature, but in optimal immune function.
Perhaps we will return to where we began and know it for the first time. But only when the power of the Pharmaceutical industry over allopathic medicine is crushed.
Thank you for the clarity of your writing, the research and all of it.